Lipoprotein(a): A Genetic Health Risk Most People Miss
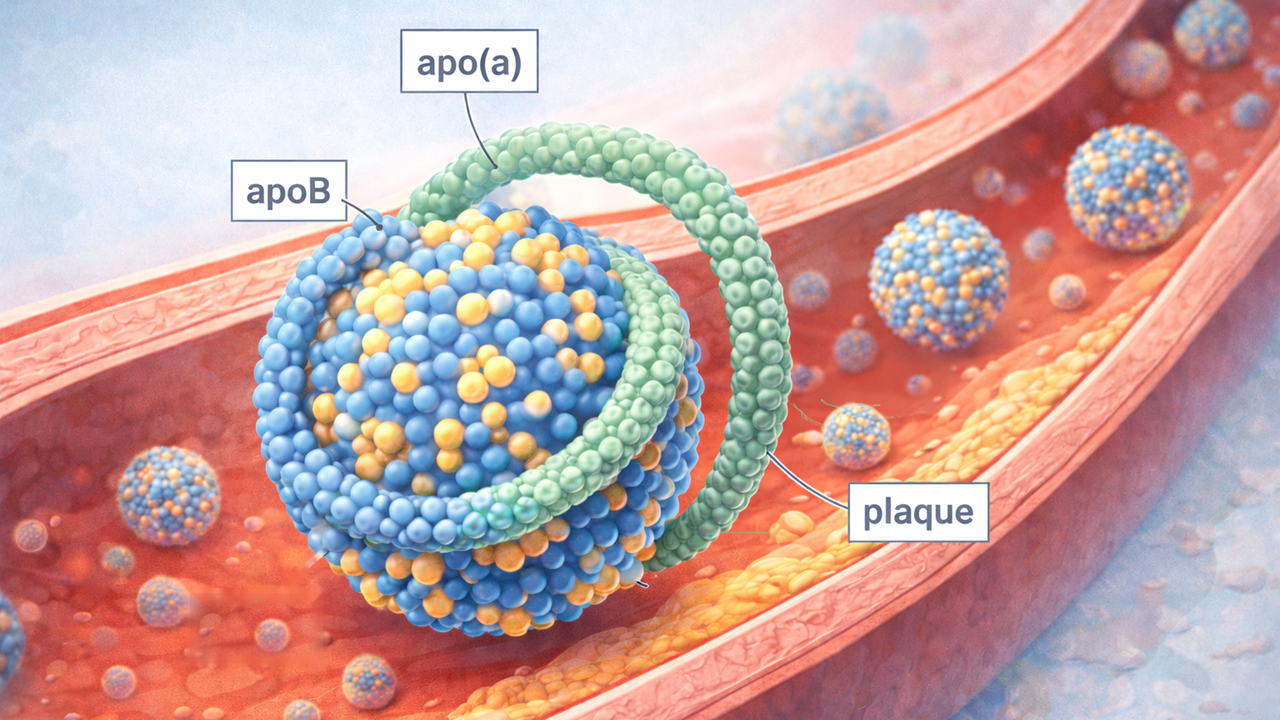
Lipoprotein(a), or Lp(a), is a genetic health risk marker hiding in plain sight. It is a cholesterol-carrying particle built from apoB-100 and apolipoprotein(a), and when levels are high, long-term risk rises for heart attack, stroke, peripheral artery disease, and aortic valve stenosis. The problem is that Lp(a) is usually not part of a standard lipid panel, high levels usually cause no symptoms, and testing rates have historically been low.
Current North American and European guidance now points in the same general direction: Lp(a) measurement belongs in cardiovascular risk assessment, and most adults should have it checked at least once in life. That does not make Lp(a) destiny, and it does not turn a blood test into a diagnosis. It does mean that one underused marker can sharpen the bigger picture of lifelong cardiovascular risk.
Why Lp(a) is a genetic health risk marker
Lp(a) is not just “extra LDL.” It is a distinct apoB-containing lipoprotein with an attached apo(a) component, and expert groups now treat elevated Lp(a) as an independent, causal cardiovascular risk factor rather than a trivial lab curiosity. That distinction matters because a person can have otherwise ordinary-looking cholesterol results and still carry additional inherited risk through Lp(a).
For most people, Lp(a) level is mostly inherited and relatively stable over time. National Lipid Association guidance notes that Lp(a) can reach adult levels early in life, while Cleveland Clinic explains that a child’s level will often resemble the level seen for years afterward. That stability is part of the reason one measurement can often be informative for a long time.
This is not a rare edge-case marker. The American Heart Association and the NLA both describe elevated Lp(a) as common, affecting about 1 in 5 people worldwide. Yet the NLA also highlights how rarely the test has been ordered in real-world U.S. practice, even in patients with known vascular disease. That gap is a big reason so many people have never heard of it.
What high Lp(a) actually means
High Lp(a) appears to add risk through more than one pathway. It can contribute to plaque buildup, promote inflammation, and increase clotting tendency. The strongest and most consistent links are with atherosclerotic cardiovascular disease, but elevated Lp(a) is also associated with stroke, peripheral artery disease, and calcific aortic valve stenosis. That last point is easy to miss in generic cholesterol articles, but it is one reason Lp(a) matters beyond the standard “heart attack risk” frame.
Another important nuance: Lp(a) behaves more like a risk continuum than a simple safe/unsafe switch. Modern guidance uses thresholds for practical decision-making, but the underlying relationship with cardiovascular risk is continuous. In plain English, a high result is meaningful, yet its practical importance still depends on the rest of the risk profile around it, including LDL-C, blood pressure, diabetes, smoking, kidney disease, and family history.
Who should consider an Lp(a) test?
The broadest answer has changed in recent years: current guidance increasingly treats Lp(a) as a once-in-adulthood measurement. The AHA’s 2026 dyslipidemia guideline summary highlights at least one lifetime test, the NLA recommends measuring Lp(a) in every adult at least once, and European guidance has supported once-in-life adult testing for years.
Testing becomes especially relevant when there is premature heart disease in the person or family, known family history of high Lp(a), familial hypercholesterolemia, recurrent cardiovascular events despite otherwise reasonable risk-factor control, or a first-degree relative with elevated Lp(a). In children, testing is usually selective rather than universal and is mainly discussed in higher-risk situations such as familial hypercholesterolemia, unexplained ischemic stroke, or strong family history.
Because Lp(a) runs strongly in families, a high result often does not stay a one-person issue. Both the AHA and the NLA support cascade-style family screening once elevated Lp(a) is identified. In practice, that means parents, siblings, and children may also need their level checked so inherited risk is not discovered only after an avoidable cardiovascular event.
How to interpret an Lp(a) result
The first thing to check is the unit. Lp(a) may be reported in nmol/L or mg/dL, but the NLA advises against converting between the two with a fixed formula because Lp(a) particles vary in size. The cleanest approach is to interpret the number in the unit the lab actually used.
A quick way to read the number
Low: under 75 nmol/L (about under 30 mg/dL).
Intermediate:75 to 125 nmol/L (about 30 to 50 mg/dL). This is the gray zone where repeat testing or closer context-based interpretation may make sense.
High:125 nmol/L and above (about 50 mg/dL and above).
Those cutoffs are useful, but they are not a verdict on their own. Modern guidance treats Lp(a) as a risk-enhancing factor that helps reclassify overall cardiovascular risk, not as a stand-alone diagnosis. It is also worth noting that average Lp(a) levels tend to be higher in some groups, including people of African descent and South Asian populations, yet the NLA states that the practical risk categories apply across races and ethnicities.
What high Lp(a) does and does not change
What can be done now
A high Lp(a) result is actionable now, but not because there is a simple Lp(a)-only fix. The actionable part is that the result can justify earlier or more intensive attention to the risk factors that are modifiable: LDL-C and other apoB-containing lipoproteins, blood pressure, diabetes, smoking, body weight, and the overall prevention strategy. That is the main clinical value of knowing the number today.
Lifestyle remains important, but with an important caveat: it usually does not meaningfully lower the Lp(a) number itself. What it does do is lower total cardiovascular risk around that inherited background. That is why exercise, diet quality, sleep, weight management, and tobacco avoidance still matter, even if the Lp(a) concentration barely moves. For the broader cardiometabolic side of that conversation, Jivaro’s related guides on cholesterol and triglyceride management, intermittent fasting, and GLP‑1 agonists for weight loss explore risk factors that sit around—rather than directly on top of—Lp(a).
As of March 2026, major AHA patient-facing materials still state that there is no medication approved just to lower Lp(a). Some PCSK9 inhibitors lower both LDL-C and Lp(a), and lipoprotein apheresis has an FDA-recognized role in a narrow, very high-risk group with familial hypercholesterolemia and established coronary or peripheral artery disease. That is a very different situation from ordinary primary prevention, which is why Lp(a) treatment discussions need context.
What is in the pipeline
The future is more promising than the present. The NLA describes pelacarsen and olpasiran as dedicated Lp(a)-lowering therapies under investigation, and by 2025–2026 pelacarsen, olpasiran, and lepodisiran were all being studied in large cardiovascular-outcome programs or event-reduction trials. What is still missing is the decisive randomized proof that specifically lowering Lp(a) leads to fewer heart attacks, strokes, or cardiovascular deaths. Until those outcome data arrive, the science remains encouraging but incomplete.
When to talk to a clinician about Lp(a)
The calm, practical moment to raise Lp(a) is when the existing risk picture feels incomplete. That includes a family history of early heart attack or stroke, known familial hypercholesterolemia, vascular disease that seems out of proportion to standard cholesterol numbers, a relative with high Lp(a), or a family pattern of unexplained early valve or artery disease. In children and teenagers, the threshold to test is usually higher and more selective.
FAQ
Is Lp(a) included in a regular cholesterol test?
Usually no. Both the AHA and Cleveland Clinic note that Lp(a) is not part of a standard lipid panel and generally needs to be ordered separately.
Can diet and exercise lower Lp(a)?
They usually do not lower the Lp(a) level much, if at all. Their value is in lowering overall cardiovascular risk around a genetically determined marker that is largely fixed.
Should family members be tested if one person has high Lp(a)?
Often yes. Major guidance supports cascade screening of first-degree relatives because elevated Lp(a) runs strongly in families.
Do results need to be repeated?
Not always. One measurement is often enough when the result is clearly low or clearly high, but the NLA notes that repeat testing can make sense in the intermediate range and in selected clinical contexts.
Are Lp(a)-lowering treatments coming?
Probably, but the key question is still outcome benefit. Dedicated therapies are in advanced studies, yet there is still no approved Lp(a)-specific drug with proven event reduction as of the current guideline era.
Conclusion
Lp(a) is one of the clearest examples of a measurable genetic health risk that modern cardiovascular medicine can identify but still often underuses. It does not replace LDL-C, blood pressure, diabetes status, smoking history, or family history. It sharpens them. For a test that usually needs to be done only once, it can materially improve how long-term cardiovascular risk is understood.
References
American Heart Association. Lipoprotein(a).
American Heart Association. What is Lipoprotein (a) and How Does It Impact My Heart Health?
National Lipid Association. A focused update to the 2019 NLA scientific statement on use of lipoprotein(a) in clinical practice.
American Heart Association. 2026 Guideline on the Management of Dyslipidemia summary.
Centers for Disease Control and Prevention. About Lipoprotein (a).
European Atherosclerosis Society / European Society of Cardiology materials on Lp(a) testing and consensus.
Cleveland Clinic. Lipoprotein (a): Levels & Testing.
Pelacarsen, olpasiran, and lepodisiran development programs and trial materials.