
Quick Answer: Supplements Studied for Improving eGFR
No over-the-counter supplement has strong evidence proving it reliably “improves eGFR” for the general public. eGFR, or estimated glomerular filtration rate, is a calculated estimate of how well the kidneys filter blood, usually based on creatinine and sometimes cystatin C. It can fluctuate because of hydration, recent diet, muscle mass, illness, medications, pregnancy, lab variation, and changes in creatinine production—not only because kidney tissue has improved or worsened.[1]
The most evidence-relevant “supplement-like” interventions are not general wellness products. Oral sodium bicarbonate or other alkali therapy has been studied in people with chronic kidney disease (CKD) and metabolic acidosis, but results are mixed and use requires monitoring for sodium load, blood pressure, swelling, and bicarbonate levels.[4][5] Ketoanalogues or ketoacid amino-acid products have been studied only as part of carefully supervised very-low-protein diets in selected CKD patients—not as standalone kidney supplements.[6]
For most supplement categories—omega-3s, probiotics, vitamin D, magnesium, CoQ10, curcumin, NAC, cranberry, creatine, protein powders, electrolytes, and herbal “kidney cleanse” products—the evidence either does not show meaningful eGFR improvement, is indirect, or is mainly about safety. People with CKD, diabetes, hypertension, kidney stones, transplant history, abnormal urine tests, or abnormal lab results should treat kidney supplements as medical-risk products rather than casual wellness add-ons.
Medical Safety Note
This guide is educational and does not recommend that any reader start, stop, combine, or change supplements. Kidney disease can be silent, and supplements can interact with ACE inhibitors, ARBs, diuretics, SGLT2 inhibitors, diabetes medicines, anticoagulants, blood-pressure medicines, transplant medicines, lithium, NSAIDs, and other drugs. People who are pregnant or breastfeeding, have CKD, diabetes, hypertension, heart failure, kidney stones, a kidney transplant, abnormal potassium, abnormal calcium, abnormal phosphorus, abnormal urine albumin, or a recent unexplained eGFR drop should review supplements with a qualified clinician, nephrologist, pharmacist, or renal dietitian before use.
Who This Guide Is For
This guide is for a broad health audience, including people who saw a borderline eGFR on lab results, people with CKD who are considering supplements, people with diabetes or hypertension trying to protect kidney function, people with a history of kidney stones, and wellness readers who have seen “kidney detox” or “raise your GFR” marketing. It is written to separate what has been studied from what is being sold.
The article uses a broad evidence map because “all supplements” can include vitamins, minerals, amino acids, botanicals, protein powders, probiotics, electrolytes, antioxidants, creatine, ketoanalogues, and multi-ingredient cleanse products. The key distinction is evidence category: some products have direct kidney-function studies in selected patients, some have indirect evidence, some are used for deficiency or CKD complications rather than eGFR, and some are mainly safety concerns.
When to Get Medical Care First
A low or changing eGFR should be interpreted with the full clinical picture. Medical care should come before supplement experimentation if there is a sudden drop in eGFR, new protein or blood in urine, foamy urine, swelling in the legs or around the eyes, shortness of breath, severe fatigue, confusion, very high blood pressure, chest pain, persistent vomiting or diarrhea, dehydration, fever with flank pain, severe back or side pain, reduced urination, or inability to urinate. These can point to acute kidney injury, infection, obstruction, kidney stones, glomerular disease, heart failure, medication toxicity, or other conditions that need evaluation.
Prompt evaluation is also important when an abnormal kidney result appears after starting or increasing NSAIDs, antibiotics, diuretics, blood-pressure medications, SGLT2 inhibitors, lithium, chemotherapy, contrast imaging, high-dose vitamins, creatine, protein powders, herbal products, or electrolyte supplements. A supplement that changes creatinine, potassium, calcium, phosphorus, fluid balance, or blood pressure can make kidney labs worse or harder to interpret.
What eGFR Is and How Kidney Function Is Usually Managed
eGFR estimates how well the kidneys filter waste from the blood. The National Kidney Foundation describes GFR as a measure of kidney filtering function and notes that measured GFR is more complex, while eGFR is widely available because it can be calculated from blood-test markers such as creatinine and, in some cases, cystatin C.[1] A commonly used staging framework treats eGFR of 90 or higher as the normal range, 60–89 as possible early kidney disease when other evidence of kidney damage exists, 15–59 as kidney disease, and below 15 as possible kidney failure.[1]
eGFR is only one kidney-health number. Urine albumin-to-creatinine ratio, or uACR, is often just as important because albumin in the urine can signal kidney damage and higher risk even when eGFR is not severely reduced. KDIGO’s CKD framework emphasizes classification and risk assessment using both GFR category and albuminuria category, along with cause of kidney disease and the patient’s overall risk profile.[2]
Kidney function is usually managed by addressing the cause and risk drivers rather than chasing a supplement effect. Evidence-based CKD care commonly includes blood-pressure control, diabetes management, individualized use of ACE inhibitors or ARBs when appropriate, SGLT2 inhibitors in many eligible CKD patients, statins for cardiovascular risk when indicated, smoking cessation, sodium reduction, individualized protein guidance, avoidance of kidney-toxic medications, correction of acidosis or anemia when present, and monitoring of potassium, bicarbonate, calcium, phosphorus, and urine albumin.[2]
How to Read the Evidence on eGFR Supplements
Supplement studies can look more promising than they are if eGFR is treated as a simple score. A real kidney-protective effect usually means slower eGFR decline over time, lower albuminuria when relevant, fewer kidney-failure events, or improved management of a defined CKD complication. A short-term eGFR rise can reflect hydration, lower creatinine production, lab variability, or reduced muscle breakdown. It does not automatically mean kidney scarring reversed.
When reading supplement claims, look for the population, outcome, and comparator. Was the study done in healthy adults, people with diabetes, people with CKD stage 3–4, dialysis patients, transplant recipients, or kidney-stone formers? Did it measure eGFR, measured GFR, creatinine, cystatin C, albuminuria, potassium, bicarbonate, phosphorus, dialysis need, or symptoms? Was the product compared with placebo, standard medical therapy, diet counseling, or no treatment?
Evidence hierarchy used here: strongest weight is given to human randomized trials, systematic reviews, clinical guidelines, and official safety resources that directly measure kidney-function outcomes. Indirect evidence is labeled as indirect. Animal-only, cell-only, marketing-only, or “detox” claims are not treated as evidence that a supplement improves eGFR.
Evidence Snapshot Table
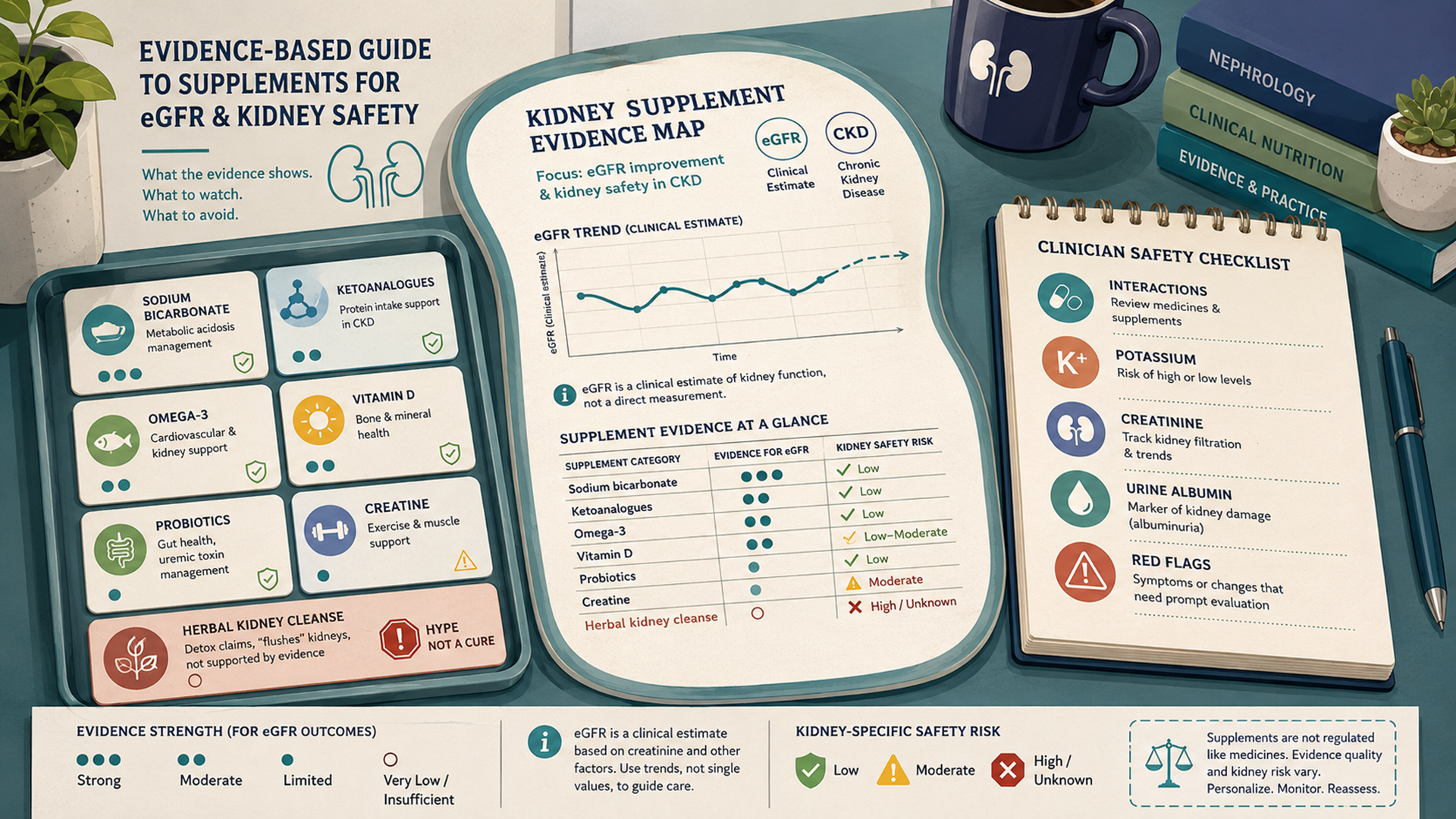
The table below maps common supplement categories by what the evidence can and cannot support. It is intentionally broad because many products are marketed for “kidney support” without direct eGFR evidence.
| Supplement category | Direct eGFR or kidney-function evidence | Most relevant context | What the evidence does not prove | Key safety caution |
|---|---|---|---|---|
| Sodium bicarbonate / alkali therapy | Direct evidence in CKD with metabolic acidosis, but results are mixed across trials.[4][5] | Low serum bicarbonate in CKD under clinician monitoring. | Does not prove baking soda is a general eGFR booster. | Sodium load, swelling, blood pressure, heart failure risk, alkalosis, and drug interactions. |
| Ketoanalogues / ketoacid amino-acid products | Direct CKD studies when combined with supervised very-low-protein diets.[6] | Selected advanced CKD patients under nephrologist and renal dietitian care. | Does not prove standalone amino-acid supplements improve eGFR. | Malnutrition risk if protein is restricted without expert supervision. |
| Omega-3 fish oil / EPA / DHA | Kidney-function evidence is mixed and not strong enough for general eGFR improvement claims. | Triglyceride management, cardiovascular-risk discussions, or disease-specific contexts. | Does not prove fish oil reverses CKD or raises eGFR. | Bleeding concerns at high doses and possible atrial fibrillation signal in some cardiovascular-trial analyses.[15][16] |
| Vitamin D / calcitriol / calcium products | Used for deficiency or CKD mineral-bone disorder; not proven as eGFR-improving supplements.[9][17] | Documented deficiency, CKD-MBD, calcium/phosphorus/PTH management. | Does not prove high-dose vitamin D improves kidney filtering. | Hypercalcemia, kidney stones, vascular calcification concerns, and toxicity from excessive dosing. |
| Iron, folate, B12, B-complex | Mostly deficiency or anemia support; not eGFR improvement evidence. | Documented deficiency, CKD anemia workup, dialysis-related losses, restricted diets. | Does not prove megadosing B vitamins improves kidney function. | Iron should not be taken without a reason; dose and route depend on labs and CKD stage. |
| Magnesium | Limited direct eGFR evidence for general use. | Documented low magnesium or clinician-directed indication. | Does not prove magnesium raises eGFR in people with normal magnesium status. | Diarrhea, accumulation in kidney disease, and dangerous high magnesium in severe cases.[10] |
| Potassium / electrolyte blends / salt substitutes | No good evidence as general eGFR improvers. | Only when potassium status and medical context support use. | Does not prove electrolyte packets improve kidney function. | Hyperkalemia risk in CKD, heart failure, ACE inhibitor/ARB use, potassium-sparing diuretics, and some diabetes or blood-pressure regimens.[11] |
| Phosphorus products / phosphate salts | No evidence as eGFR-improving supplements. | Rare deficiency scenarios or clinician-directed replacement. | Does not prove phosphorus supports kidney function. | High phosphorus is commonly a CKD management concern, especially in later stages. |
| Probiotics, prebiotics, synbiotics | Some CKD trials target uremic toxins or gut microbiome markers, but eGFR benefit is not established.[8] | Research settings, gut symptoms, or specific strain/product rationale. | Does not prove “a probiotic” improves eGFR. | Infection risk in severely ill or immunocompromised people; strain effects are not interchangeable. |
| CoQ10, NAC, curcumin, resveratrol, antioxidants | Mostly indirect, condition-specific, or mixed; NAC did not prevent major contrast-related outcomes in a large angiography trial.[7] | Specific clinician-guided situations, not routine eGFR improvement. | Does not prove antioxidant supplements regenerate kidney function. | Drug interactions, bleeding risk, liver concerns, kidney stones with high-oxalate products, and variable product quality. |
| Creatine | No evidence as an eGFR-improving supplement; may complicate creatinine-based eGFR interpretation. | Sports nutrition in healthy users, not kidney treatment.[14] | Does not prove kidney protection; a creatinine change may not equal true GFR change. | Caution with CKD, abnormal labs, diabetes, hypertension, nephrotoxic drugs, or dehydration risk. |
| Protein powders, collagen, essential amino acids | No evidence as general eGFR improvers; protein needs depend on CKD stage and dialysis status.[13] | Nutrition support when protein intake is inadequate or dialysis increases needs. | Does not prove more protein improves kidney function. | Excess protein may be inappropriate in non-dialysis CKD; too little protein can also be harmful. |
| Cranberry, D-mannose, urinary-tract supplements | Usually studied for urinary symptoms or UTI prevention, not eGFR improvement. | Recurrent UTI discussions in selected people. | Does not prove kidney filtering improves. | Stone history, sugar content, anticoagulant use, and delayed care for kidney infection symptoms. |
| Herbal “kidney cleanse,” detox teas, diuretic herbs | No credible evidence that cleanse products improve eGFR. | Generally not a kidney-function strategy. | Does not prove detoxification, stone prevention, or CKD reversal. | Contaminants, aristolochic acid, high potassium/phosphorus, diuretic effects, and transplant-drug interactions.[12] |
Supplement-by-Supplement Evidence
Sodium Bicarbonate and Alkali Therapy
Sodium bicarbonate is one of the few supplement-like products with direct CKD and eGFR-related research, but it is not a general kidney booster. The rationale applies mainly to metabolic acidosis, a condition in which blood bicarbonate is low and acid load is higher than the kidneys can manage. In a 2009 randomized trial of CKD patients with low bicarbonate, bicarbonate supplementation was associated with slower creatinine-clearance decline and fewer patients progressing rapidly, but the trial population was specific and the intervention was medically monitored.[4]
The picture is not uniformly positive. The BiCARB trial in older adults with advanced CKD and low-grade acidosis found no improvement in physical function or kidney function and more adverse events with bicarbonate than placebo.[5] The practical takeaway is that bicarbonate may be appropriate for selected CKD patients with low bicarbonate, but it should be guided by serum bicarbonate, blood pressure, swelling, sodium intake, heart failure risk, and medication review—not by the desire to make eGFR look higher.
Ketoanalogues and Very-Low-Protein Diets
Ketoanalogues, sometimes called ketoacid amino-acid supplements, are not typical wellness supplements. They are used in some CKD nutrition strategies alongside very-low-protein diets to reduce nitrogen waste while trying to prevent malnutrition. In a randomized trial, a ketoanalogue-supplemented vegetarian very-low-protein diet was studied in patients with advanced CKD, but this kind of approach requires careful dietitian and nephrology oversight.[6]
This is not the same as buying amino acids online for “kidney support.” Protein restriction can be harmful when done incorrectly, especially in older adults, people losing weight unintentionally, people with poor appetite, people with inflammation, and people on dialysis who may need more protein rather than less. Ketoanalogue strategies belong in clinical nutrition, not self-directed supplement experimentation.
Omega-3 Fish Oil, EPA, DHA, and Algae Oil
Omega-3 supplements are often marketed for heart and inflammation support, which makes them appealing to people with kidney concerns. The kidney-specific evidence, however, does not support a broad claim that fish oil improves eGFR. Omega-3s may be relevant for triglyceride management or certain disease-specific discussions, but eGFR improvement is not a dependable outcome for general users.[15]
Safety also matters. Higher-dose marine omega-3 products have been associated with increased atrial fibrillation risk in a meta-analysis of randomized cardiovascular outcome trials.[16] People taking anticoagulants, preparing for surgery, managing arrhythmias, or using prescription omega-3 products should discuss dose and purpose with a clinician.
Vitamin D, Calcitriol, Calcium, and CKD Mineral-Bone Health
Vitamin D is important in kidney care, but not because it reliably raises eGFR. CKD can disrupt mineral metabolism, parathyroid hormone regulation, calcium balance, phosphorus balance, and bone health. Vitamin D testing or treatment may be appropriate for deficiency or CKD mineral-bone disorder, and active vitamin D medications may be used in selected patients, but that is a different question from using vitamin D as an eGFR supplement.[9][17]
High-dose vitamin D or calcium can be harmful. Excess vitamin D can cause hypercalcemia, and high calcium levels can contribute to kidney stones, kidney injury, and calcification problems. People with CKD, kidney stones, sarcoidosis, hyperparathyroidism, high calcium, high phosphorus, or abnormal parathyroid hormone should not use high-dose vitamin D or calcium products without lab-guided care.[9]
Iron, B Vitamins, Folate, and B12
Iron, folate, vitamin B12, and some B-complex vitamins may be relevant when a deficiency, anemia, restricted diet, dialysis-related loss, or specific clinical indication exists. In CKD, anemia evaluation often includes iron status and other contributors. Correcting a deficiency can improve symptoms and blood markers, but it does not mean the supplement improves eGFR.
Iron is a good example of why “kidney support” language can be misleading. Iron may be necessary for iron-deficiency anemia, but unnecessary iron can cause gastrointestinal side effects and may be unsafe in certain iron-overload states. The right decision depends on hemoglobin, ferritin, transferrin saturation, inflammation, CKD stage, dialysis status, symptoms, and clinician guidance.
Magnesium
Magnesium is involved in muscle, nerve, bone, and cardiovascular function, but direct evidence that magnesium supplements improve eGFR is limited. Magnesium may be useful when deficiency is documented or when a clinician recommends it for a specific reason, but routine use for eGFR is not evidence-based.
Kidney safety is the main issue. Healthy kidneys help clear excess magnesium, but people with impaired kidney function are more vulnerable to accumulation. High supplemental magnesium can cause diarrhea, nausea, low blood pressure, weakness, confusion, and abnormal heart rhythm in severe toxicity.[10] Magnesium-containing laxatives and antacids also count toward total exposure.
Potassium, Electrolytes, and Salt Substitutes
Potassium is essential for normal muscle and heart function, but potassium supplementation is one of the riskiest areas for people with kidney concerns. CKD, heart failure, dehydration, ACE inhibitors, ARBs, potassium-sparing diuretics, some diabetes medicines, and some antibiotics can raise hyperkalemia risk. The National Kidney Foundation notes that people with high potassium may be advised to limit high-potassium foods, while people with low potassium may need the opposite approach.[11]
That is why electrolyte powders, coconut-water powders, potassium citrate products, salt substitutes, and “hydration” mixes need context. They do not improve eGFR simply because they contain electrolytes. They may be appropriate for certain athletes or dehydration scenarios, but they can be dangerous for people with CKD, abnormal potassium, heart failure, blood-pressure medications, or kidney-stone regimens that already include citrate therapy.
Phosphorus Products and Phosphate Salts
Phosphorus is another mineral where more is not automatically better. In CKD, high phosphorus can become a management problem, especially in advanced disease and dialysis. Phosphate supplements are usually relevant only for documented deficiency or specific clinician-directed treatment, not for improving eGFR.
Multi-mineral products, bone-health stacks, bodybuilding products, enemas, and some bowel-prep products can contain phosphate or other mineral loads that matter for kidney patients. People with CKD should review phosphorus sources with a clinician or renal dietitian, especially when lab results show high phosphorus, abnormal parathyroid hormone, or CKD mineral-bone disorder.
Probiotics, Prebiotics, and Synbiotics
The gut-kidney connection is a real research area. Some CKD studies evaluate whether probiotics, prebiotics, or synbiotics can alter gut-derived uremic toxins, inflammation, constipation, or microbiome patterns. In the SYNERGY trial, a synbiotic intervention changed some uremic toxin measures, but this does not translate into a proven eGFR-improvement claim for probiotic products generally.[8]
Probiotics are not interchangeable. A product’s effect depends on strain, dose, viability, duration, and patient population. People who are immunocompromised, critically ill, recently transplanted, have central venous catheters, or are taking immunosuppressants should not assume probiotics are automatically safe.
NAC, CoQ10, Curcumin, Resveratrol, and Antioxidants
Antioxidants are often marketed as kidney-protective because oxidative stress is involved in many kidney diseases. But antioxidant biology does not prove that an antioxidant capsule improves eGFR. N-acetylcysteine, or NAC, is a useful example: it was widely studied for contrast-associated kidney injury prevention, but the large PRESERVE trial found no benefit of oral acetylcysteine or sodium bicarbonate over placebo or saline strategy for major angiography-related kidney outcomes.[7]
CoQ10, curcumin, resveratrol, green tea extract, alpha-lipoic acid, and similar products may have small studies in inflammation, blood pressure, diabetes, oxidative stress, or proteinuria-related markers, but they should not be presented as proven eGFR improvers. Safety issues vary: curcumin and fish-oil combinations may matter for bleeding risk; green tea extract can be a liver concern at high doses; high-dose vitamin C can increase oxalate and kidney-stone concerns in susceptible people; and multi-ingredient antioxidant products are hard to evaluate.
Creatine
Creatine is a sports-nutrition supplement, not a kidney-function supplement. In healthy people using standard doses, creatine has a relatively strong sports-nutrition evidence base, but that does not mean it improves eGFR.[14] Because many eGFR equations use serum creatinine, and creatine can influence creatinine production, creatine can complicate interpretation of creatinine-based kidney labs.
A higher creatinine after creatine use does not always mean true kidney damage, but it also should not be ignored. People with CKD, diabetes, hypertension, kidney stones, abnormal urine albumin, dehydration risk, or nephrotoxic medication exposure should discuss creatine before use and should tell clinicians if they are taking it before interpreting labs.
Protein Powders, Collagen, Essential Amino Acids, and BCAAs
Protein is necessary for health, but protein needs change by kidney stage, nutrition status, and dialysis status. The National Kidney Foundation notes that people with kidney disease who are not on dialysis may be advised to limit protein, while people on dialysis often need more protein because dialysis removes protein waste and increases nutritional demands.[13]
Protein powders, collagen, amino-acid blends, and BCAA products do not improve eGFR simply by supporting muscle. In non-dialysis CKD, excess protein may be inappropriate for some patients. At the same time, unnecessary restriction can cause malnutrition. The safe middle ground is individualized dietitian-guided protein planning, not generic “kidney support” powder.
Cranberry, D-Mannose, and Urinary-Tract Supplements
Cranberry, D-mannose, and urinary-tract blends are usually marketed for urinary tract infection support, not eGFR. Preventing recurrent lower urinary symptoms is a different outcome from improving kidney filtering. A kidney infection, fever with flank pain, blood in urine, pregnancy with urinary symptoms, or recurrent infections needs medical evaluation rather than supplement-only management.
People with kidney stones should be cautious with high-dose cranberry or vitamin C products because oxalate burden may matter for some stone formers. People taking anticoagulants should also ask about cranberry products because medication interactions are sometimes a concern.
Herbal “Kidney Cleanse,” Detox Teas, Diuretic Herbs, and Botanicals
Herbal kidney products are among the highest-risk categories because evidence is often weak and product quality is variable. The National Kidney Foundation warns that herbal supplements can worsen kidney disease, interact with prescription medicines, contain contaminants such as heavy metals, contain kidney-damaging ingredients such as aristolochic acid, or accumulate to toxic levels in people with kidney disease.[12]
Products such as dandelion, horsetail, nettle, parsley root, uva ursi, licorice, aloe taken by mouth, cat’s claw, chaparral, comfrey, yohimbe, St. John’s wort, and traditional multi-herb formulas may carry risks for people with CKD, dialysis, transplant history, autoimmune kidney disease, high potassium, medication interactions, or unclear product sourcing.[12] “Detox” language should be viewed skeptically: kidneys do not need a cleanse product to filter blood, and a diuretic effect is not the same as improved kidney function.
Safety, Interactions, and Who Should Be Careful
Supplement safety is more complicated in kidney health because the kidneys regulate fluid balance, acid-base status, electrolytes, mineral balance, waste removal, and drug clearance. The FDA defines dietary supplements broadly to include vitamins, minerals, herbs, botanicals, amino acids, live microbials, and other dietary substances, but it does not approve most dietary supplements for safety and effectiveness before marketing.[3]
| Situation | Supplements to review first | Why it matters |
|---|---|---|
| CKD stage 3–5, dialysis, or transplant history | Herbs, magnesium, potassium, phosphorus, vitamin D, calcium, probiotics, creatine, protein powders, antioxidants. | Clearance, electrolyte balance, immunosuppression, and medication interactions can change risk. |
| ACE inhibitors, ARBs, spironolactone, eplerenone, finerenone, trimethoprim, or potassium supplements | Potassium, salt substitutes, electrolyte powders, coconut-water powders, herbal potassium sources. | These combinations can increase hyperkalemia risk. |
| Diuretics, vomiting, diarrhea, heat illness, fasting, or dehydration risk | Creatine, high-dose caffeine, detox teas, diuretic herbs, magnesium laxatives, electrolyte blends. | Fluid shifts can cause acute kidney injury or misleading creatinine changes. |
| Kidney stones or high urine oxalate | High-dose vitamin C, cranberry concentrates, turmeric/curcumin, high-dose vitamin D/calcium. | Some products can increase oxalate or calcium-related stone concerns in susceptible people. |
| High calcium, high phosphorus, abnormal PTH, or CKD mineral-bone disorder | Vitamin D, calcium, phosphorus, bone-health stacks, mineral blends. | Mineral balance in CKD requires lab-guided management. |
| Anticoagulants or upcoming surgery | Fish oil, turmeric/curcumin, garlic, ginkgo, vitamin E, cranberry, multi-herb products. | Bleeding risk and perioperative planning should be reviewed. |
| Pregnancy or breastfeeding | Herbal detox products, high-dose vitamins/minerals, creatine, weight-loss products, stimulant blends. | Safety data may be limited, and kidney-related symptoms in pregnancy need clinical evaluation. |
| High blood pressure or heart failure | Sodium bicarbonate, licorice, stimulants, high-sodium electrolytes, salt tablets. | Sodium load, fluid retention, and blood-pressure effects can be clinically important. |
What the Research Does Not Prove
The research does not prove that supplements can regenerate scarred kidney tissue, reverse CKD, eliminate the need for evidence-based medication, or make eGFR rise safely in every person. It also does not prove that a supplement that lowers creatinine has improved true GFR. Creatinine is part of many eGFR equations, so anything that changes muscle mass, protein intake, creatine use, hydration, or creatinine production can change eGFR interpretation.
The research also does not prove that supplement stacks are better than single products. Multi-ingredient “kidney support” blends often combine herbs, minerals, diuretics, antioxidants, electrolytes, and proprietary extracts. If kidney labs change after starting a stack, it may be difficult to tell whether the change came from hydration, creatinine production, potassium load, contaminants, blood-pressure effects, or actual kidney injury.
How to Talk to a Clinician About Supplements and eGFR
A useful clinician conversation starts with the lab pattern, not the product. Bring the supplement label, dose, frequency, start date, and reason for use. Also bring recent eGFR results, creatinine, cystatin C if available, urine albumin-to-creatinine ratio, potassium, bicarbonate, calcium, phosphorus, blood pressure, A1C if diabetic, and a complete medication list.
Useful questions include:
- Is my eGFR change likely real, or could it reflect hydration, creatine, muscle mass, medication, or lab variation?
- Do I also have albumin or blood in the urine?
- Should my kidney function be repeated, or should cystatin C be used to confirm the estimate?
- Do I have metabolic acidosis, anemia, high potassium, high phosphorus, vitamin D deficiency, or another condition where supplementation is medically relevant?
- Could this supplement interact with my ACE inhibitor, ARB, diuretic, SGLT2 inhibitor, diabetes medicine, anticoagulant, NSAID use, or transplant medicine?
- What symptom or lab change would mean I should stop the supplement and call?
How to Choose Supplements More Safely
Safer supplement selection begins with skepticism toward disease-treatment claims. Avoid products that claim to “reverse kidney disease,” “cleanse the kidneys,” “flush toxins,” “raise GFR fast,” or replace prescribed kidney medication. These claims are especially concerning when the product contains proprietary blends, undisclosed doses, stimulant ingredients, diuretic herbs, or minerals that affect potassium, magnesium, calcium, or phosphorus.
Look for transparent ingredient amounts, third-party testing where available, lot number, expiration date, allergen information, and a product that lists every active ingredient clearly. Third-party testing does not prove a supplement improves eGFR, but it can reduce some quality concerns. Avoid starting several supplements at once, because side effects and lab changes become much harder to interpret.
Common Mistakes to Avoid
- Chasing a single eGFR result. A trend plus urine albumin and clinical context is more useful than one number.
- Assuming “natural” means kidney-safe. Herbal supplements can contain contaminants, high potassium, high phosphorus, or kidney-toxic compounds.[12]
- Using creatine without telling the clinician. It can complicate creatinine-based eGFR interpretation.
- Adding electrolytes because eGFR is low. Potassium, sodium, magnesium, and phosphorus can be risky in CKD.
- Taking high-dose vitamin D or calcium without labs. Excess can cause hypercalcemia and kidney-stone or kidney-injury concerns.[9]
- Using protein powders without knowing CKD stage or dialysis status. Protein needs are individualized and can go in opposite directions depending on context.[13]
- Delaying care for red flags. Blood in urine, swelling, severe flank pain, fever, low urine output, or a sudden eGFR drop should be evaluated medically.
FAQ
Can supplements improve eGFR?
No over-the-counter supplement has strong evidence showing it reliably improves eGFR in the general population. Some medically directed interventions have been studied in selected CKD groups, but eGFR is not a supplement score to chase.
What supplement has the best evidence for kidney function?
The most relevant evidence is for sodium bicarbonate in CKD with metabolic acidosis and ketoanalogues as part of supervised very-low-protein diets. Both require clinical oversight and are not general kidney supplements.[4][6]
Can creatine lower eGFR?
Creatine can raise serum creatinine in some users, and creatinine is used to calculate many eGFR results. That can make eGFR interpretation harder without necessarily proving kidney damage, but abnormal labs should still be reviewed.
Are kidney cleanse supplements safe?
Kidney cleanse products are not proven to improve eGFR and can be risky. Herbal products may contain contaminants, high potassium or phosphorus, kidney-toxic ingredients, or compounds that interact with medications.[12]
Should people with CKD take vitamin D?
Some people with CKD need vitamin D testing or treatment, but vitamin D is not an eGFR booster. Dose should depend on deficiency, calcium, phosphorus, parathyroid hormone, CKD stage, and clinician guidance.[9][17]
What labs matter besides eGFR?
Urine albumin-to-creatinine ratio, creatinine trend, cystatin C when needed, potassium, bicarbonate, calcium, phosphorus, blood pressure, diabetes markers, and urine findings can all change the interpretation of kidney risk.[1][2]
Sources and Evidence Method
This article prioritized kidney-specific clinical evidence, current CKD guidance, official supplement-safety resources, and human studies that measured kidney-function outcomes. Evidence was categorized as direct when a supplement or supplement-like intervention was tested against kidney-function outcomes such as eGFR, measured GFR, creatinine clearance, albuminuria, kidney failure, or CKD progression; indirect when the supplement affected related issues such as inflammation, triglycerides, deficiency, acidosis, anemia, mineral balance, or gut-derived toxins without proving eGFR improvement; and safety-only when the product was included because it is commonly marketed for kidney health but has meaningful kidney risk.
Because supplement evidence can become outdated or product-specific, the article avoids ranking commercial products and avoids affiliate-style recommendations. A trial of one formulation, one dose, or one patient population should not be generalized to every brand, blend, or person with abnormal kidney labs.
Author, Reviewer, and Last Updated
References
- National Kidney Foundation. (2026). Estimated glomerular filtration rate (eGFR).
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. (2024). KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney International, 105(4S), S117–S314.
- U.S. Food and Drug Administration. (2022). Questions and answers on dietary supplements.
- de Brito-Ashurst, I., Varagunam, M., Raftery, M. J., & Yaqoob, M. M. (2009). Bicarbonate supplementation slows progression of CKD and improves nutritional status. Journal of the American Society of Nephrology, 20(9), 2075–2084.
- Witham, M. D., Band, M. M., Littleford, R. C., Avenell, A., Soiza, R. L., McMurdo, M. E. T., Sumukadas, D., Ogston, S. A., Lamb, E. J., Hampson, G., & Struthers, A. D. (2020). Bicarbonate supplementation for older people with chronic kidney disease and low-grade acidosis: A randomised, double-blind, placebo-controlled trial. BMC Medicine, 18, 91.
- Garneata, L., Stancu, A., Dragomir, D., Stefan, G., & Mircescu, G. (2016). Ketoanalogue-supplemented vegetarian very low-protein diet and CKD progression. Journal of the American Society of Nephrology, 27(7), 2164–2176.
- Weisbord, S. D., Gallagher, M., Jneid, H., Garcia, S., Cass, A., Thwin, S. S., Conner, T. A., Chertow, G. M., Bhatt, D. L., Shunk, K., Parikh, C. R., McFalls, E. O., Brophy, M., Ferguson, R., Wu, H., Androsenko, M., Myles, J., Kaufman, J., Palevsky, P. M., & PRESERVE Trial Group. (2018). Outcomes after angiography with sodium bicarbonate and acetylcysteine. The New England Journal of Medicine, 378(7), 603–614.
- Rossi, M., Johnson, D. W., Morrison, M., Pascoe, E. M., Coombes, J. S., Forbes, J. M., Szeto, C.-C., McWhinney, B. C., Ungerer, J. P. J., Campbell, K. L., & SYNERGY Study Group. (2016). Synbiotics easing renal failure by improving gut microbiology: A randomized controlled trial. Clinical Journal of the American Society of Nephrology, 11(2), 223–231.
- National Institutes of Health Office of Dietary Supplements. (2024). Vitamin D: Fact sheet for health professionals.
- National Institutes of Health Office of Dietary Supplements. (2022). Magnesium: Fact sheet for health professionals.
- National Kidney Foundation. (2025). Potassium in your CKD diet.
- National Kidney Foundation. (2025). “Kidney detox” and herbal supplements: What’s safe and what’s not.
- National Kidney Foundation. (2025). CKD diet: How much protein is the right amount?.
- Kreider, R. B., Kalman, D. S., Antonio, J., Ziegenfuss, T. N., Wildman, R., Collins, R., Candow, D. G., Kleiner, S. M., Almada, A. L., & Lopez, H. L. (2017). International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14, 18.
- National Institutes of Health Office of Dietary Supplements. (2024). Omega-3 fatty acids: Fact sheet for health professionals.
- Gencer, B., Djousse, L., Al-Ramady, O. T., Cook, N. R., Manson, J. E., Albert, C. M., & Gaziano, J. M. (2021). Effect of long-term marine omega-3 fatty acids supplementation on the risk of atrial fibrillation in randomized controlled trials of cardiovascular outcomes. Circulation, 144(25), 1981–1990.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. (2017). KDIGO 2017 clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder. Kidney International Supplements, 7(1), 1–59.