
Quick Answer: Supplements Studied for Extending Lifespan
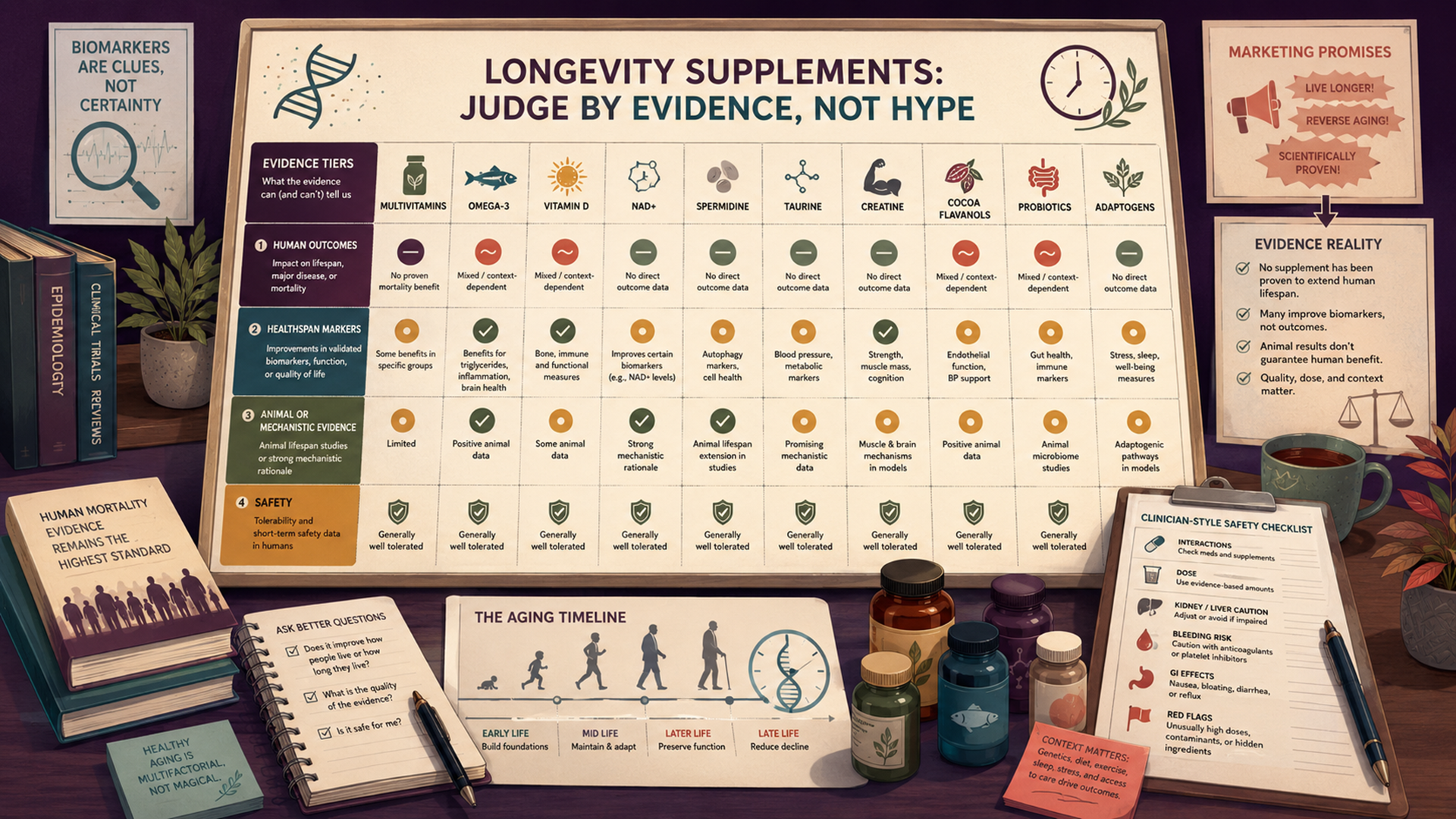
No over-the-counter supplement has strong evidence proving it extends human lifespan in generally healthy adults. Some supplements have been studied for mortality-related outcomes, such as multivitamins, vitamin D, omega-3 fatty acids, and cocoa flavanols. Others—such as NAD+ precursors, spermidine, taurine, creatine, protein, CoQ10, glycine/N-acetylcysteine, berberine, curcumin, resveratrol, quercetin, fisetin, probiotics, and adaptogens—are mainly supported by biomarker, healthspan, disease-specific, animal, or mechanistic evidence rather than direct proof of longer human life.[1][2]
The most important distinction is lifespan versus healthspan. Lifespan means how long someone lives. Healthspan refers to the years lived with good function, mobility, cognition, independence, and lower disease burden. A supplement might improve a biomarker, support a deficiency, or help maintain muscle when combined with resistance training, but that does not prove it extends life. A true lifespan claim needs human mortality or survival evidence, not just “anti-aging” language.
For a broad health audience, the evidence supports a cautious answer: supplements may be useful for correcting deficiencies, supporting specific medical or nutrition needs, or improving selected healthspan-related outcomes. But “longevity stacks” and “life-extension supplements” often overstate animal studies, short biomarker trials, or observational associations. People with cancer history, kidney or liver disease, pregnancy or breastfeeding, bleeding risk, diabetes medicines, immune suppression, arrhythmias, psychiatric medications, or upcoming surgery should treat longevity supplements as medically relevant products, not casual wellness add-ons.
Medical Safety Note
This guide is educational and does not recommend that any reader start, stop, combine, or change supplements. Supplements can interact with prescription medicines, affect bleeding risk, alter blood sugar, affect liver or kidney function, and complicate surgery or pregnancy care. The U.S. Food and Drug Administration does not approve dietary supplements for safety and effectiveness before they are marketed in the same way it reviews drugs, and FDA advises consumers to speak with a doctor, pharmacist, or other health professional before using supplements because some can interact with medicines or other supplements.[1]
Who This Guide Is For
This guide is for readers who want a factual overview of supplements studied for extending lifespan or supporting healthy aging. It is also for people who see claims about NAD+, spermidine, taurine, resveratrol, fisetin, quercetin, creatine, omega-3s, vitamin D, or “anti-aging stacks” and want to know what the research actually shows.
The article uses a broad evidence map rather than a “top 10 longevity supplements” ranking. That matters because longevity claims are often built from different types of evidence: a human mortality study, a biomarker trial, a study in older adults, an animal lifespan study, a cell-culture mechanism, or a marketing claim. Those are not equivalent.
When to Get Medical Care First
Supplement decisions should not delay medical care. Get professional evaluation before experimenting with longevity supplements if there is unexplained weight loss, persistent fatigue, anemia, blood in stool or urine, chest pain, fainting, severe palpitations, new shortness of breath, jaundice, severe abdominal pain, rapid swelling, confusion, new neurologic symptoms, recurrent falls, severe insomnia, worsening depression, suicidal thoughts, or symptoms that started after a new supplement.
Medical review is also important for people with cancer history, liver disease, kidney disease, heart rhythm disorders, bleeding disorders, diabetes, autoimmune disease, transplant history, seizure disorder, bipolar disorder, pregnancy or breastfeeding, fertility treatment, or upcoming surgery. These contexts can change the risk-benefit balance for common longevity-marketed supplements, including fish oil, vitamin D, curcumin, berberine, melatonin, adaptogens, antioxidants, probiotics, and electrolyte or mineral products.
What Lifespan and Healthspan Mean—and How Healthy Aging Is Usually Supported
Lifespan is the total length of life. Healthspan is the portion of life spent in relatively good health, with preserved function and lower disability. A supplement can be relevant to healthy aging without being proven to extend lifespan. For example, creatine may support strength gains when combined with resistance training, and vitamin D may be necessary for people with deficiency, but neither fact proves a universal life-extension effect.
Healthy aging is usually supported by addressing the major drivers of disability and mortality: blood pressure, smoking, diabetes, cardiovascular risk, cancer screening where appropriate, vaccination, sleep, nutrition, muscle strength, mobility, fall prevention, social connection, hearing and vision, mental health, medication review, and management of chronic disease. Supplements sometimes fit into that picture when they correct a deficiency or support a defined goal, but they do not replace evidence-based care.
This is also why prescription longevity topics should be kept separate from supplements. Metformin, rapamycin, GLP-1 medications, statins, aspirin, and hormone therapy are not dietary supplements. They have medical uses, risks, contraindications, and monitoring needs. They should not be self-used for lifespan extension because they are discussed in longevity circles.
How to Read the Evidence on Longevity Supplements
Longevity evidence should be sorted by outcome. The strongest evidence for “extending lifespan” would come from randomized human trials or very strong human data showing lower all-cause mortality or longer survival. This is rare because lifespan trials require large numbers of people and long follow-up. The next tier is disease-specific outcomes, such as cardiovascular events, cancer outcomes, fractures, hospitalization, or frailty. Below that are biomarkers, such as inflammation, NAD+ levels, glucose, LDL cholesterol, muscle mass, methylation clocks, telomere length, or mitochondrial markers.
Animal lifespan studies are scientifically valuable but easy to overuse in marketing. A compound can extend lifespan in yeast, worms, flies, or mice and still fail to extend lifespan in humans. The biology may not translate, the human dose may be unsafe, the effect may depend on genetic background or diet, or the animal outcome may reflect a stress response that is not desirable in people.
Evidence hierarchy used here: human mortality and clinical-outcome evidence first; then healthspan and disease-risk evidence; then biomarker evidence; then animal or mechanistic evidence. Animal-only or cell-only findings are not treated as proof that a supplement extends human lifespan.
Evidence Snapshot Table
The table below summarizes common supplements marketed for longevity. It separates direct human outcome evidence from biomarker, animal, mechanistic, limited, or safety-only evidence.
| Supplement category | Evidence tier | What research suggests | What it does not prove | Key safety caution |
|---|---|---|---|---|
| Multivitamins | Human mortality evidence | A 2024 analysis of 390,124 generally healthy U.S. adults found no mortality benefit from daily multivitamin use.[3] | Does not support taking multivitamins to live longer. | May still be useful for specific deficiency or dietary gaps; excess iron, vitamin A, or other nutrients can be harmful. |
| Vitamin D and calcium | Human outcome and deficiency evidence | Useful for deficiency or bone-related indications; VITAL did not show broad primary prevention of cancer or cardiovascular events with vitamin D in generally healthy adults.[4] | Does not prove high-dose vitamin D extends lifespan. | Excess vitamin D can cause hypercalcemia; calcium and vitamin D need caution in kidney stones, kidney disease, and high calcium states.[18] |
| Omega-3 fatty acids: fish oil, EPA, DHA, algae oil | Human clinical-outcome evidence | VITAL did not show a broad reduction in major cardiovascular events or cancer with 1 g/day marine omega-3 in generally healthy adults, although some subgroup and secondary findings remain debated.[5] | Does not prove fish oil extends lifespan in healthy adults. | Higher-dose marine omega-3s have been linked with increased atrial fibrillation risk in cardiovascular-outcome trials.[6] |
| Cocoa flavanols | Human outcome and biomarker evidence | COSMOS found no significant reduction in total cardiovascular events, but a secondary cardiovascular-death signal was reported and remains hypothesis-generating.[7] | Does not prove cocoa extract extends lifespan or that chocolate has the same effect. | Chocolate products vary widely in flavanol content and may contain sugar, calories, and contaminants. |
| Fiber supplements and prebiotic fibers | Human diet-outcome evidence; supplement evidence indirect | Higher dietary fiber intake is associated with lower mortality and cardiometabolic risk in large reviews, but this does not automatically prove fiber pills extend lifespan.[8] | Does not prove a specific fiber supplement increases lifespan. | Fiber can worsen bloating, interact with medication absorption, and needs careful use in bowel obstruction or severe GI disease. |
| Protein, collagen, essential amino acids, HMB | Healthspan evidence | Protein adequacy and resistance training support muscle health in older adults; some supplements may help when intake is low or frailty risk is high.[9] | Does not prove high-protein supplementation extends lifespan. | Kidney disease, liver disease, cancer cachexia, dialysis, and frailty require individualized nutrition guidance. |
| Creatine | Healthspan and sports-nutrition evidence | Creatine has evidence for strength and lean-mass support, especially with resistance training, but not for human lifespan extension.[10] | Does not prove creatine slows aging or extends life. | Can complicate creatinine-based kidney lab interpretation; caution with kidney disease or abnormal labs. |
| NAD+ precursors: nicotinamide riboside, NMN | Biomarker evidence | Human studies show some NAD+ precursors can raise NAD-related markers, but clinical benefits remain uncertain.[11] | Does not prove longer lifespan, cancer prevention, or disease prevention. | Long-term safety, product quality, dosing, and regulatory status require caution. |
| Spermidine | Observational human diet evidence; animal/mechanistic evidence | Higher dietary spermidine intake has been linked to lower mortality in observational research, and animal work suggests autophagy-related mechanisms.[12] | Does not prove spermidine supplements extend human lifespan. | Supplement doses, purity, cancer-history considerations, and long-term safety are not settled. |
| Taurine | Animal lifespan evidence; human uncertainty | A 2023 Science study reported taurine-related aging effects in animals, but human lifespan benefit is unproven.[13] | Does not prove taurine supplements slow aging in people. | High-dose, long-term use lacks robust safety evidence; energy drinks add caffeine and other ingredients. |
| GlyNAC: glycine plus N-acetylcysteine | Small human healthspan/biomarker trials | Small trials in older adults have reported changes in glutathione, oxidative stress, and functional markers, but the evidence is early.[14] | Does not prove lifespan extension. | NAC can interact with medications and may not be appropriate around some procedures or bleeding-risk contexts. |
| CoQ10 | Disease-specific evidence | CoQ10 has been studied in heart failure and selected older populations, but findings are not a general longevity recommendation.[15] | Does not prove healthy adults live longer with CoQ10. | May interact with anticoagulants and can cause digestive symptoms. |
| Berberine | Metabolic biomarker evidence | Berberine has been studied for glucose and lipid markers, but not as a proven lifespan supplement. | Does not prove life extension or cardiovascular-event reduction. | Can interact with diabetes medicines, anticoagulants, antibiotics, immunosuppressants, and pregnancy-related safety concerns. |
| Curcumin, resveratrol, quercetin, fisetin, polyphenol extracts | Mechanistic, animal, and biomarker evidence | These compounds are often studied for inflammation, senescence, oxidative stress, or metabolic markers, but human lifespan data are lacking. | Does not prove senolytic or anti-aging benefit in people. | Concentrated extracts can affect bleeding, liver enzymes, drug metabolism, and surgery planning. |
| Melatonin | Sleep/circadian evidence; no lifespan proof | Melatonin is relevant to circadian timing and some sleep contexts, not proven lifespan extension.[19] | Does not prove anti-aging benefit from nightly use. | Long-term use, pregnancy, children, sedatives, seizure disorders, and product-label accuracy require caution. |
| Probiotics and synbiotics | Condition-specific and gut-brain/gut-immune evidence | Some strains help specific GI or antibiotic-associated contexts; lifespan evidence is not established.[20] | Does not prove microbiome supplements extend life. | Rare infections have occurred in severely ill or immunocompromised people. |
| Adaptogens and botanicals: ashwagandha, rhodiola, ginseng, saffron | Stress/sleep biomarker evidence; limited longevity evidence | Some products have small stress or sleep studies, but not human lifespan proof. | Does not prove “stress resilience” equals longevity. | Ashwagandha should be avoided in pregnancy and has been linked to rare liver-injury reports.[21] |
Supplement-by-Supplement Evidence
Multivitamins and Broad Vitamin-Mineral Formulas
Multivitamins are the most familiar “insurance policy” supplement, but they are not proven lifespan extenders. The U.S. Preventive Services Task Force concluded in 2022 that evidence was insufficient to assess the balance of benefits and harms of multivitamin supplementation for preventing cardiovascular disease or cancer in nonpregnant community-dwelling adults, and recommended against beta carotene or vitamin E for that purpose.[2] A 2024 JAMA Network Open study of 390,124 generally healthy adults found that daily multivitamin use was not associated with a mortality benefit.[3]
This does not mean multivitamins are never useful. They may help in specific situations such as restricted diets, malabsorption, pregnancy planning, bariatric surgery, or documented nutrient gaps. But the evidence does not support using a multivitamin as a general life-extension strategy.
Vitamin D and Calcium
Vitamin D is important for calcium absorption, bone health, and deficiency correction, but it is frequently oversold as a longevity supplement. In the VITAL randomized trial, vitamin D3 supplementation did not significantly reduce invasive cancer or major cardiovascular events in generally healthy middle-aged and older adults over the main trial period.[4] Some secondary or subgroup findings have generated interest, but they do not establish vitamin D as a lifespan-extending supplement.
Safety depends on dose and context. Excess vitamin D can cause high calcium levels, which can lead to nausea, weakness, confusion, kidney stones, kidney injury, and abnormal heart rhythm in severe cases.[18] Calcium supplements also require caution in kidney stones, kidney disease, high calcium, cardiovascular-risk discussions, and people already receiving calcium-rich diets.
Omega-3 Fatty Acids
Omega-3 fatty acids are often discussed for cardiovascular health, inflammation, triglycerides, and brain aging. In VITAL, 1 gram per day of marine omega-3 fatty acids did not significantly reduce major cardiovascular events or cancer in the overall generally healthy trial population.[5] That does not erase all possible cardiovascular relevance, but it weakens simple claims that fish oil makes healthy adults live longer.
Omega-3 safety is not trivial. Higher-dose marine omega-3 products, especially in cardiovascular outcome trials, have been associated with increased atrial fibrillation risk.[6] People with arrhythmias, bleeding risk, anticoagulant use, upcoming surgery, fish allergy, or prescription omega-3 therapy should clarify dose and purpose with a clinician.
Cocoa Flavanols and Polyphenol-Rich Extracts
Cocoa flavanols are among the more interesting supplement categories because they have human outcome data from the COSMOS trial. COSMOS did not find a statistically significant reduction in total cardiovascular events for cocoa extract, but it did report a lower cardiovascular-death signal as a secondary outcome.[7] That is promising but not definitive proof of lifespan extension.
This also does not mean eating more chocolate reproduces trial conditions. Chocolate products vary in flavanol content and may contain sugar, saturated fat, calories, cadmium, lead, or other contaminants depending on sourcing and processing. A cocoa-flavanol capsule used in a trial is not the same as a candy bar.
Fiber Supplements and Prebiotic Fibers
Higher dietary fiber intake is consistently associated with lower all-cause mortality and lower cardiometabolic risk in large evidence reviews.[8] That makes fiber one of the most credible “healthy aging” nutrition targets. But the evidence is strongest for dietary patterns rich in fiber-containing foods, not necessarily for a single fiber powder extending lifespan.
Supplemental fiber can still be useful when it helps someone meet intake targets, improve constipation, support LDL cholesterol reduction, or manage glucose response. Psyllium, inulin, resistant starch, partially hydrolyzed guar gum, acacia fiber, and beta-glucan products are not interchangeable. Fiber can worsen bloating, constipation, diarrhea, reflux, or medication absorption if introduced too quickly or without enough fluid.
Protein, Collagen, Essential Amino Acids, HMB, and Creatine
Muscle is central to healthspan. Low muscle mass and strength are linked with frailty, falls, disability, and loss of independence. Protein adequacy and resistance training are therefore more credible healthy-aging strategies than most “anti-aging” supplements. Expert groups have argued that many older adults may need more protein than the basic adult RDA, depending on health status, physical activity, and clinical context.[9]
Creatine is one of the better-studied sports-nutrition supplements for strength and lean-mass outcomes, especially when combined with resistance training.[10] But muscle support is not the same as lifespan extension. Creatine can also complicate interpretation of creatinine-based kidney labs, and high-protein or amino-acid strategies may be inappropriate in some kidney, liver, cancer, dialysis, or frailty contexts.
NAD+ Precursors: Nicotinamide Riboside and NMN
NAD+ biology is real. NAD+ participates in energy metabolism, DNA repair, and cellular stress responses, and NAD-related pathways are a legitimate aging-research area. Human studies show that nicotinamide riboside and related precursors can raise NAD-related markers in some contexts.[11] But raising a biomarker does not prove longer life, lower disease risk, or slower biological aging.
The main evidence gap is clinical outcomes. NAD+ precursor trials are generally too short and too small to show lifespan effects. Regulatory status, product purity, dose, long-term safety, cancer-history questions, and interactions with other therapies remain important. NAD+ IV drips, injections, and high-dose stacks should not be treated as proven anti-aging care.
Spermidine
Spermidine is a polyamine found in foods such as wheat germ, soybeans, legumes, mushrooms, and aged cheese. Observational research has linked higher dietary spermidine intake with lower mortality, and animal studies suggest possible mechanisms involving autophagy and cardiometabolic pathways.[12]
The key limitation is that observational dietary intake is not supplement proof. People who consume more spermidine-rich foods may also have different overall diets, lifestyles, socioeconomic factors, and health behaviors. Supplement trials have not proven that spermidine capsules extend human lifespan. People with cancer history or complex medical conditions should be especially cautious with supplements marketed around cell growth, autophagy, or “cell renewal.”
Taurine
Taurine drew major attention after animal research suggested links between taurine status and aging phenotypes, including lifespan effects in some species.[13] The finding is scientifically interesting, but it is not a human longevity prescription. Animal lifespan effects are often not reproduced in people, and human taurine patterns may depend on age, sex, diet, kidney function, metabolic status, and measurement context.
Taurine also appears in energy drinks, but energy drinks are not taurine supplements in isolation. They may contain caffeine, sugar, stimulants, and other ingredients that affect blood pressure, sleep, palpitations, anxiety, and arrhythmia risk. A taurine headline should not become a reason to use high-dose energy products for aging.
GlyNAC: Glycine plus N-Acetylcysteine
GlyNAC combines glycine and N-acetylcysteine, two precursors used by the body to make glutathione. Small human trials in older adults have reported changes in oxidative stress, mitochondrial markers, inflammation, insulin resistance, and some functional measures.[14] These are healthspan-related signals, not proof of lifespan extension.
NAC has medication and safety considerations, including possible interactions around blood pressure, bleeding-risk contexts, nitroglycerin, asthma sensitivity in some people, and perioperative planning. Glycine and NAC can also cause gastrointestinal effects. Multi-ingredient “mitochondrial” or “detox” blends are harder to evaluate than single-ingredient trials.
CoQ10 and Selenium
CoQ10 is involved in mitochondrial electron transport and has been studied in heart failure, statin-associated muscle symptoms, migraine, and older-adult cardiovascular contexts. A heart-failure trial and a Swedish study combining selenium and CoQ10 reported disease-specific or population-specific signals, but these findings do not establish CoQ10 as a universal longevity supplement for healthy adults.[15]
CoQ10 may interact with anticoagulants such as warfarin and can cause gastrointestinal symptoms. Selenium is also dose-sensitive; excessive selenium can cause hair and nail changes, gastrointestinal symptoms, neurologic symptoms, and other toxicity concerns. CoQ10-selenium trial results should not be generalized to people who are not similar to the studied population.
Berberine
Berberine is commonly marketed as a metabolic and “longevity” supplement because it has been studied for glucose, lipid, and AMPK-related pathways. But metabolic biomarker changes are not the same as demonstrated survival benefit. There is no strong human evidence that berberine extends lifespan.
Berberine also has drug-like interaction potential. It may interact with diabetes medicines, anticoagulants, blood-pressure medications, immunosuppressants, antibiotics, and pregnancy-related safety contexts. People should not treat berberine as a harmless alternative to prescribed metabolic care.
Curcumin, Resveratrol, Quercetin, Fisetin, and Senolytic-Marketed Products
Curcumin, resveratrol, quercetin, and fisetin are often marketed around inflammation, oxidative stress, sirtuins, senescence, or “cellular cleanup.” Some have animal or mechanistic evidence and small human biomarker studies. None has robust human evidence proving lifespan extension.
Senolytic language is especially easy to overstate. Removing senescent cells in animal models is a real research area, but a supplement advertised as “senolytic” does not automatically reproduce experimental drug effects. Concentrated extracts can interact with anticoagulants, cancer therapies, liver enzymes, and surgery planning. Curcumin and green tea extracts have also been linked with rare liver-injury concerns in supplement contexts.
Melatonin
Melatonin is a hormone involved in circadian timing. It can be relevant for jet lag, delayed sleep timing, or selected sleep conversations, but it is not a proven lifespan supplement. Better sleep can support healthspan, but that does not mean melatonin itself slows aging.[19]
Long-term nightly use should not be assumed risk-free. Melatonin products may contain more or less melatonin than the label states, and some analyses have found product-content variability.[22] Pregnancy, breastfeeding, children, seizure disorders, autoimmune disease, depression, bipolar disorder, sedatives, and anticoagulants deserve clinician review.
Probiotics, Prebiotics, and Synbiotics
The gut microbiome is involved in metabolism, immune signaling, inflammation, and drug metabolism, so microbiome science is relevant to aging. But probiotics are strain-specific interventions, not a single category with one effect. Evidence for lifespan extension in humans is not established.[20]
Probiotics may be useful in certain gastrointestinal or antibiotic-associated contexts, but people who are severely ill, immunocompromised, recently transplanted, hospitalized, or have central venous catheters should not assume they are automatically safe. Prebiotics and synbiotics can also worsen bloating, gas, diarrhea, or constipation in some people.
Adaptogens and Botanicals
Ashwagandha, rhodiola, ginseng, saffron, valerian, lion’s mane, medicinal mushrooms, and many traditional botanical formulas are marketed for stress resilience, sleep, immunity, hormones, or cognitive aging. Some have small trials for specific symptoms. That is not the same as human lifespan evidence.
Botanicals can be pharmacologically active. Ashwagandha is not recommended during pregnancy and has been linked to rare liver-injury reports.[21] St. John’s wort has major drug-interaction risks. Ginseng, ginkgo, garlic, turmeric, and mushroom extracts may interact with anticoagulants, immunosuppressants, diabetes medicines, psychiatric medications, cancer therapies, and surgery planning.
Prescription Longevity Topics Are Not Supplements
Metformin, rapamycin, GLP-1 medications, statins, aspirin, and hormone therapy are frequently discussed in longevity communities. They should not be grouped with supplements. These are prescription or drug-like medical interventions with approved uses, contraindications, side effects, monitoring needs, and sometimes strong disease-specific evidence.
A drug that lowers mortality in a high-risk disease group does not automatically become a longevity drug for healthy people. Statins, for example, are used based on cardiovascular-risk assessment, not as general anti-aging supplements. Rapamycin has notable animal-longevity data, but it is an immune-modulating prescription drug. GLP-1 medications may reduce cardiovascular events in selected high-risk populations, but they are not supplements and should not be used from unregulated sources.
Safety, Interactions, and Who Should Be Careful
Longevity supplements are often taken by people who are also taking medications or managing chronic conditions. That is exactly when supplement risk rises. The table below highlights common caution zones.
| Situation | Supplements to review first | Why it matters |
|---|---|---|
| Pregnancy, trying to conceive, or breastfeeding | High-dose vitamins, botanicals, ashwagandha, berberine, melatonin, NAD+ precursors, “hormone support” blends. | Safety data may be limited, and some botanicals or high-dose compounds may be inappropriate. |
| Cancer history or active cancer treatment | High-dose antioxidants, spermidine, NAD+ boosters, mushroom extracts, curcumin, resveratrol, quercetin, fisetin. | Some supplements may interact with therapy, affect metabolism, or make unproven cell-growth or autophagy claims. |
| Kidney disease or abnormal kidney labs | Creatine, high protein, magnesium, potassium, vitamin D, calcium, electrolyte blends, high-dose vitamin C. | Kidney function affects clearance and electrolyte balance; creatine can complicate creatinine-based labs. |
| Liver disease or elevated liver enzymes | Ashwagandha, green tea extract, kava, curcumin, multi-herb blends, high-dose niacin. | Some supplements have been linked to liver injury or may stress drug-metabolism pathways. |
| Bleeding risk, anticoagulants, antiplatelet drugs, or surgery | Fish oil, garlic, ginkgo, turmeric/curcumin, vitamin E, resveratrol, nattokinase, serrapeptase. | Bleeding risk and perioperative planning may change. |
| Diabetes or glucose-lowering medications | Berberine, cinnamon, alpha-lipoic acid, chromium, bitter melon, high-dose niacin. | Blood sugar may fall too low or medication effects may be harder to manage. |
| Immune suppression, transplant medicines, biologics, or autoimmune disease | Probiotics, medicinal mushrooms, echinacea, ashwagandha, high-dose immune blends. | Immune effects, infection risk, and drug interactions can matter clinically. |
| Arrhythmias, palpitations, anxiety, insomnia, or stimulant sensitivity | High caffeine, yohimbine, synephrine, energy products, thyroid-support blends, high-dose omega-3s. | Some products can affect heart rhythm, heart rate, blood pressure, anxiety, or sleep. |
| Psychiatric medications or seizure history | 5-HTP, tryptophan, St. John’s wort, melatonin, ashwagandha, kava, sedating blends. | Serotonin, sedation, seizure threshold, mood cycling, and drug metabolism may be affected. |
What the Research Does Not Prove
The research does not prove that a supplement stack can override poor sleep, smoking, uncontrolled blood pressure, untreated diabetes, heavy alcohol use, inactivity, loneliness, or lack of medical care. It also does not prove that changing a biological-age test, methylation clock, inflammatory marker, NAD+ level, or glucose marker automatically translates into longer life.
The research also does not prove that “natural” compounds are safer than drugs. Natural compounds can be biologically active, contaminated, mislabeled, or combined in doses never studied together. The FDA notes that supplement manufacturers are responsible for ensuring products are not adulterated or misbranded, but FDA generally does not approve dietary supplements before they reach consumers.[1]
Finally, animal lifespan data cannot be casually converted into human recommendations. Yeast, worms, flies, and mice are powerful research models, but humans are longer-lived, genetically diverse, environmentally variable, and usually taking other medications or managing other conditions by older age.
How to Talk to a Clinician About Supplements for Longevity
A productive conversation starts with goals. “I want to live longer” is too broad to guide safe supplement use. A more useful approach is to ask what measurable problem is being addressed: deficiency, high LDL cholesterol, high triglycerides, low muscle mass, poor sleep, constipation, glucose control, frailty, bone health, anemia, inflammation, or medication side effects.
Useful questions include:
- Is there a deficiency or diagnosis this supplement is meant to address?
- Does this supplement have human outcome evidence, or only biomarker, animal, or mechanistic evidence?
- Could it interact with my medications or medical conditions?
- Is it safe with pregnancy, breastfeeding, surgery, cancer history, kidney disease, liver disease, or bleeding risk?
- What dose and duration were actually studied?
- What symptom, side effect, or lab change should make me stop and call?
- Is there a food, exercise, sleep, or medical-care strategy with better evidence for the same goal?
How to Choose Supplements More Safely
Safer supplement selection starts with avoiding products that promise to “reverse aging,” “reset biological age,” “activate immortality genes,” “cleanse senescent cells,” or “extend lifespan clinically” without human outcome evidence. Disease-treatment claims are also a warning sign because supplements are not allowed to be marketed as products that diagnose, treat, cure, or prevent disease unless regulated as drugs.[1]
Look for transparent ingredient amounts, a full Supplement Facts panel, third-party testing when available, a lot number, expiration date, allergen information, and a manufacturer that does not hide behind proprietary blends. Third-party testing does not prove lifespan benefit, but it can reduce some quality concerns. Start with one product at a time when medically appropriate; multi-supplement stacks make side effects and lab changes harder to interpret.
Common Mistakes to Avoid
- Confusing biomarkers with lifespan. A lower inflammatory marker or higher NAD+ level does not prove longer life.
- Overgeneralizing animal lifespan studies. A mouse, worm, or yeast result is not a human recommendation.
- Using high-dose antioxidants because aging involves oxidative stress. Some antioxidant supplements have failed prevention trials or raised safety concerns.
- Stacking too many products. Multiple supplements increase interaction risk and make results impossible to interpret.
- Ignoring deficiency testing. Vitamin D, iron, B12, and magnesium decisions often need clinical context rather than guessing.
- Assuming prescription longevity drugs are supplements. Rapamycin, metformin, statins, GLP-1 medications, aspirin, and hormone therapy are medical interventions.
- Buying based on influencer protocols. A personal stack is not evidence and may reflect different genetics, labs, diagnoses, medications, or risk tolerance.
- Delaying care for red flags. Chest pain, fainting, jaundice, severe abdominal pain, blood loss, sudden neurologic symptoms, or suicidal thoughts need medical evaluation.
FAQ
Can supplements extend human lifespan?
No over-the-counter supplement has strong evidence proving it extends lifespan in generally healthy adults. Some supplements affect healthspan-related markers, but that is not the same as mortality proof.
What supplement has the strongest human longevity evidence?
There is no universally proven lifespan supplement. Multivitamins have not shown a mortality benefit in a large 2024 cohort study, while vitamin D, omega-3s, and cocoa flavanols have mixed or context-specific outcome data.[3][4][5][7]
Are NAD+ supplements proven anti-aging treatments?
No. NAD+ precursors can raise NAD-related markers in some studies, but they have not been proven to extend human lifespan or prevent age-related disease.[11]
Do taurine or spermidine supplements make people live longer?
Not proven. Taurine has animal lifespan evidence, and spermidine has observational dietary-intake evidence, but randomized human supplement trials have not shown lifespan extension.[12][13]
Is creatine a longevity supplement?
Creatine is better described as a muscle and performance supplement. It may support strength and lean mass with resistance training, but it is not proven to extend lifespan.[10]
Are longevity stacks safe?
Not automatically. Stacks can combine drug-like compounds, stimulants, minerals, botanicals, and antioxidants in ways that have not been studied together. Medication interactions and liver, kidney, bleeding, pregnancy, and surgery risks should be reviewed.
Sources and Evidence Method
This article prioritized human mortality data, randomized trials, systematic reviews, government safety resources, and major clinical or nutrition references. Evidence was classified as human outcome evidence when studies measured mortality or major disease events; healthspan evidence when studies measured strength, frailty, cognition, cardiometabolic health, or function; biomarker evidence when studies measured lab or physiologic markers; animal/mechanistic evidence when findings came from model organisms or cellular pathways; and safety-only evidence when a product was included because it is commonly marketed for longevity but has meaningful risk or weak human data.
The article avoids product rankings, affiliate-style recommendations, and “best longevity supplement” claims because supplement effects depend on deficiency status, dose, baseline diet, age, sex, disease history, medication use, and product quality. References were selected to support key evidence and safety claims rather than to exhaust every mechanistic paper in aging biology.
Author, Reviewer, and Last Updated
References
- U.S. Food and Drug Administration. (2024). Questions and answers on dietary supplements.
- U.S. Preventive Services Task Force. (2022). Vitamin, mineral, and multivitamin supplementation to prevent cardiovascular disease and cancer: US Preventive Services Task Force recommendation statement. JAMA, 327(23), 2326–2333.
- Loftfield, E., O’Connell, C. P., Abnet, C. C., Graubard, B. I., Liao, L. M., Beane Freeman, L. E., Hofmann, J. N., Freedman, N. D., & Sinha, R. (2024). Multivitamin use and mortality risk in 3 prospective US cohorts. JAMA Network Open, 7(6), e2418729.
- Manson, J. E., Cook, N. R., Lee, I.-M., Christen, W., Bassuk, S. S., Mora, S., Gibson, H., Gordon, D., Copeland, T., D’Agostino, D., Friedenberg, G., Ridge, C., Bubes, V., Giovannucci, E. L., Willett, W. C., & Buring, J. E. (2019). Vitamin D supplements and prevention of cancer and cardiovascular disease. The New England Journal of Medicine, 380(1), 33–44.
- Manson, J. E., Cook, N. R., Lee, I.-M., Christen, W., Bassuk, S. S., Mora, S., Gibson, H., Gordon, D., Copeland, T., D’Agostino, D., Friedenberg, G., Ridge, C., Bubes, V., Giovannucci, E. L., Willett, W. C., & Buring, J. E. (2019). Marine n−3 fatty acids and prevention of cardiovascular disease and cancer. The New England Journal of Medicine, 380(1), 23–32.
- Gencer, B., Djoussé, L., Al-Ramady, O. T., Cook, N. R., Manson, J. E., Albert, C. M., & Gaziano, J. M. (2021). Effect of long-term marine omega-3 fatty acids supplementation on the risk of atrial fibrillation in randomized controlled trials of cardiovascular outcomes. Circulation, 144(25), 1981–1990.
- Sesso, H. D., Manson, J. E., Aragaki, A. K., Rist, P. M., Johnson, L. G., Friedenberg, G., Copeland, T., Clar, A., Mora, S., Moorthy, M. V., Bubes, V., & Wang, L. (2022). Effect of cocoa flavanol supplementation for the prevention of cardiovascular disease events: The COcoa Supplement and Multivitamin Outcomes Study randomized clinical trial. The American Journal of Clinical Nutrition, 115(6), 1490–1500.
- Reynolds, A., Mann, J., Cummings, J., Winter, N., Mete, E., & Te Morenga, L. (2019). Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. The Lancet, 393(10170), 434–445.
- Bauer, J., Biolo, G., Cederholm, T., Cesari, M., Cruz-Jentoft, A. J., Morley, J. E., Phillips, S., Sieber, C., Stehle, P., Teta, D., Visvanathan, R., Volpi, E., & Boirie, Y. (2013). Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. Journal of the American Medical Directors Association, 14(8), 542–559.
- Kreider, R. B., Kalman, D. S., Antonio, J., Ziegenfuss, T. N., Wildman, R., Collins, R., Candow, D. G., Kleiner, S. M., Almada, A. L., & Lopez, H. L. (2017). International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14, 18.
- Martens, C. R., Denman, B. A., Mazzo, M. R., Armstrong, M. L., Reisdorph, N., McQueen, M. B., Chonchol, M., & Seals, D. R. (2018). Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nature Communications, 9, 1286.
- Kiechl, S., Pechlaner, R., Willeit, P., Notdurfter, M., Paulweber, B., Willeit, K., Werner, P., Ruckenstuhl, C., Iglseder, B., Weger, S., Mairhofer, E., Mayr, M., Schroeder, S., Nairz, M., Zoller, H., Datz, C., Zangerle, A., Riml, C., Huber, A., ... Madeo, F. (2018). Higher spermidine intake is linked to lower mortality: A prospective population-based study. The American Journal of Clinical Nutrition, 108(2), 371–380.
- Singh, P., Gollapalli, K., Mangiola, S., Schranner, D., Yusuf, M. A., Chamoli, M., Shi, S. L., Lopes Bastos, B., Nair, T., Riermeier, A., Han, Y., Bechtold, M., et al. (2023). Taurine deficiency as a driver of aging. Science, 380(6649), eabn9257.
- Kumar, P., Liu, C., Suliburk, J., Hsu, J. W., Muthupillai, R., Jahoor, F., Minard, C. G., Taffet, G. E., Sekhar, R. V. (2021). Glycine and N-acetylcysteine supplementation in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition. Clinical and Translational Medicine, 11(3), e372.
- Mortensen, S. A., Rosenfeldt, F., Kumar, A., Dolliner, P., Filipiak, K. J., Pella, D., Alehagen, U., Steurer, G., Littarru, G. P., & Q-SYMBIO Study Investigators. (2014). The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: Results from Q-SYMBIO. JACC: Heart Failure, 2(6), 641–649.
- Alehagen, U., Johansson, P., Björnstedt, M., Rosén, A., & Dahlström, U. (2013). Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and coenzyme Q10 supplementation: A 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. International Journal of Cardiology, 167(5), 1860–1866.
- National Institutes of Health Office of Dietary Supplements. (2024). Omega-3 fatty acids: Fact sheet for health professionals.
- National Institutes of Health Office of Dietary Supplements. (2024). Vitamin D: Fact sheet for health professionals.
- National Center for Complementary and Integrative Health. (2025). Melatonin: What you need to know.
- National Center for Complementary and Integrative Health. (2025). Probiotics: Usefulness and safety.
- National Center for Complementary and Integrative Health. (2024). Ashwagandha: Usefulness and safety.
- Erland, L. A. E., & Saxena, P. K. (2017). Melatonin natural health products and supplements: Presence of serotonin and significant variability of melatonin content. Journal of Clinical Sleep Medicine, 13(2), 275–281.