
Quick Answer: Supplements Studied for Weight Loss
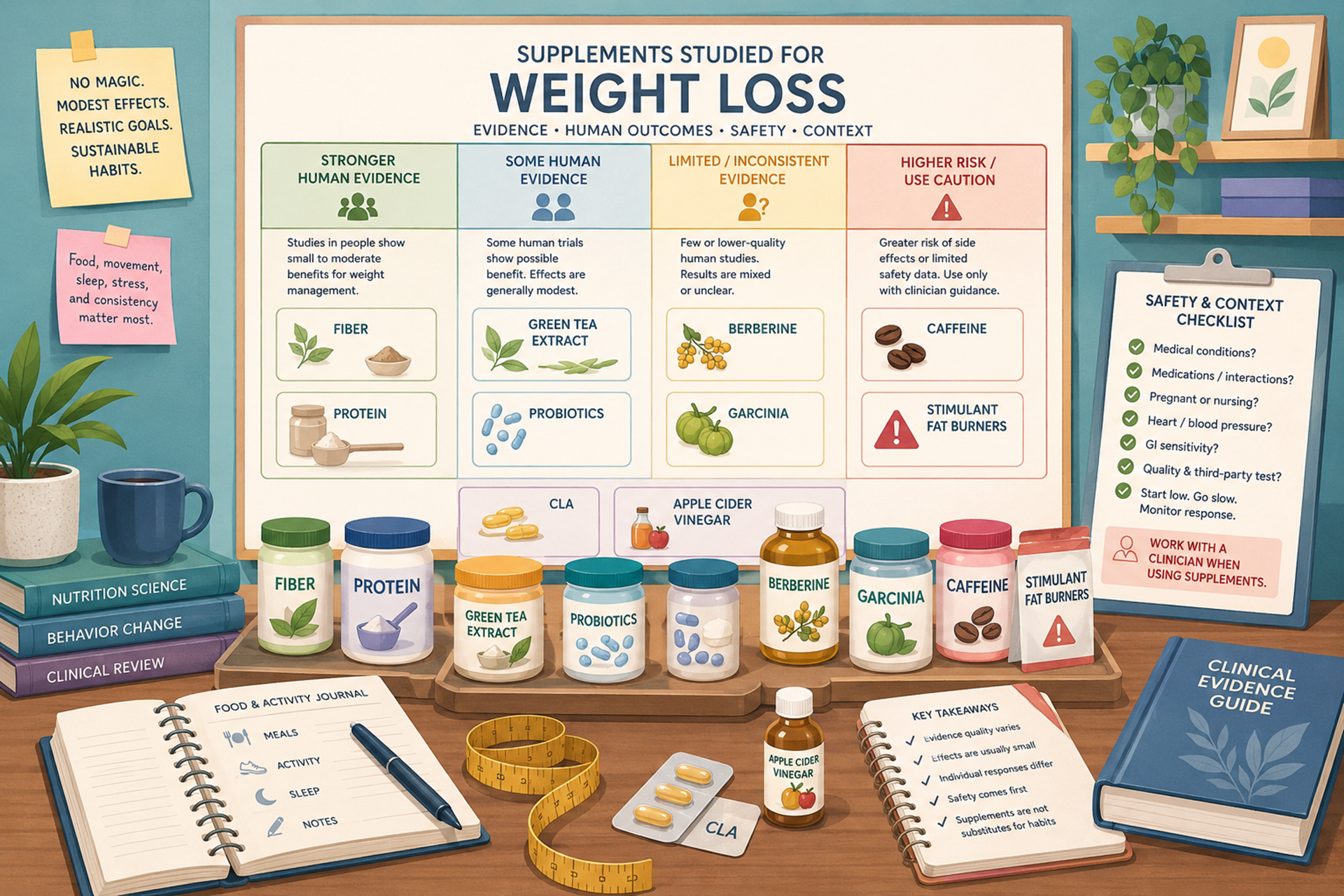
No dietary supplement reliably produces large, durable weight loss for most people. Some supplements have human evidence for small changes in body weight, waist circumference, appetite, or body composition, but the average effects are usually modest and depend heavily on diet, activity, sleep, medication use, health conditions, and the product studied. The National Institutes of Health Office of Dietary Supplements notes that weight-loss supplement ingredients vary widely in evidence quality, and many studies are small, short, methodologically limited, or difficult to interpret because products often contain multiple ingredients.[1]
The most reasonable categories to discuss are soluble fiber, protein or meal-replacement support, caffeine-containing products, green tea or green tea extract, and selected metabolic supplements such as berberine—but none should be treated as a substitute for an individualized weight-management plan. Other popular products, including garcinia cambogia, CLA, chromium, apple cider vinegar, MCT oil, detox teas, yohimbe, bitter orange, and stimulant “fat burners,” either have weak evidence, very small effects, or meaningful safety concerns.[1]
Prescription weight-loss medicines and bariatric procedures are not supplements. GLP-1 medications, orlistat, phentermine/topiramate, naltrexone/bupropion, metformin, and metabolic or bariatric surgery require medical supervision and should not be replaced by supplement products. NIDDK notes that prescription weight-management medications are used as part of a weight-control program and that medication choice depends on likely benefits, side effects, current health issues, other medications, family history, and cost.[4]
Medical Safety Note
This guide is educational and does not recommend that any reader start, stop, combine, or change supplements. Weight-loss supplements can affect blood pressure, heart rhythm, blood sugar, sleep, anxiety, liver enzymes, kidney function, digestion, hydration, and medication safety. FDA advises consumers to talk with a doctor, pharmacist, or other health professional before using dietary supplements because some supplements can interact with medicines or other supplements.[2] People who are pregnant or breastfeeding, adolescents, older adults, people with eating disorder history, diabetes, hypertension, heart disease, arrhythmias, liver disease, kidney disease, psychiatric conditions, seizures, bleeding risk, or upcoming surgery should be especially cautious.
Who This Guide Is For
This guide is for readers who want a factual map of weight-loss supplement evidence rather than a product ranking. It is also for people comparing supplement claims with medical options, including GLP-1 medications, orlistat, or bariatric care. The goal is to separate human weight-loss evidence from appetite claims, glucose claims, thermogenesis claims, detox claims, and safety concerns.
The article uses a broad definition of “weight-loss supplements” because commercial products often include vitamins, minerals, botanicals, fibers, amino acids, caffeine sources, probiotics, protein powders, green tea extracts, “carb blockers,” “fat blockers,” detox teas, and stimulant blends. That does not mean all of these are equally useful or safe. It means they should be evaluated in a consistent evidence framework.
When to Get Medical Care First
Weight-loss supplements should not be used to delay evaluation for unexplained symptoms. Medical care should come first if weight loss is rapid or unintentional, if there is chest pain, fainting, severe palpitations, shortness of breath, very high blood pressure, severe anxiety or panic symptoms, confusion, jaundice, dark urine, severe abdominal pain, persistent vomiting, blood in stool, dehydration, or severe diarrhea. These symptoms may reflect heart, liver, endocrine, gastrointestinal, psychiatric, infectious, medication-related, or eating-disorder-related problems.
Professional care is also important when weight concerns involve binge eating, purging, laxative use, extreme restriction, overexercise, body-image distress, missed periods, dizziness with standing, or fear of eating. A supplement plan can be unsafe if the underlying issue is an eating disorder, thyroid disease, diabetes medication mismatch, depression, sleep apnea, medication-induced weight gain, polycystic ovary syndrome, menopause-related body-composition change, chronic pain, or another medical factor.
What Healthy Weight Loss Means—and How Weight Management Is Usually Supported
Healthy weight loss is not simply the fastest possible drop on a scale. For some people, weight management is about reducing cardiometabolic risk, improving mobility, lowering blood pressure, improving sleep apnea, reducing joint pain, lowering triglycerides, or managing type 2 diabetes risk. For others, especially people with normal weight, eating disorder risk, pregnancy, chronic illness, or unintended weight loss, weight loss may not be medically appropriate.
Obesity is a chronic medical condition for many people, not a character flaw. NIDDK describes obesity as a chronic disease and notes that a healthy eating plan and regular physical activity can help with long-term weight control, while medications may be considered when lifestyle changes are not enough for some people.[4] The USPSTF concludes with moderate certainty that offering or referring adults with obesity to intensive, multicomponent behavioral interventions has a moderate net benefit; many effective programs aim for at least 5% weight loss and include diet, physical activity, self-monitoring, problem solving, and maintenance support.[3]
This context matters because a supplement can appear to “work” when the real driver is a calorie deficit, increased protein, reduced alcohol intake, better sleep, more activity, medication changes, or water loss. Good weight-management care looks at the whole pattern: nutrition quality, appetite, muscle preservation, mental health, medications, sleep, cardiometabolic risk, and sustainability.
How to Read the Evidence on Weight-Loss Supplements
The strongest evidence for a weight-loss supplement is a human randomized controlled trial or systematic review that directly measures body weight, BMI, waist circumference, body fat, or weight maintenance. Evidence is weaker when it measures only appetite hormones, glucose, insulin, fat oxidation, thermogenesis, gut microbiome changes, or animal weight gain. Those biomarkers can be interesting, but they do not prove meaningful weight loss in real life.
Several details matter when reading studies. Was the supplement tested alone or inside a multi-ingredient formula? Was the comparison placebo or an active diet program? Did both groups receive the same calorie target and activity support? How long was the study? How many people dropped out? Were participants already using medications? Was body composition measured, or only scale weight? Did the study report adverse events, blood pressure, liver markers, glucose, and medication interactions?
Evidence hierarchy used here: human weight-loss outcomes first; then modest or indirect evidence for appetite, glucose, lipid, thermogenesis, or body-composition markers; then limited/no evidence; then safety-only concerns. Animal-only and mechanism-only findings are not treated as proof that a supplement causes weight loss in people.
Evidence Snapshot Table
The table below gives a broad evidence map. It includes supplements with some direct human weight-loss evidence, supplements with mainly indirect evidence, and products that are common in the marketplace but mainly belong in a safety-caution category.
| Supplement category | Evidence tier | What research suggests | What it does not prove | Key safety caution |
|---|---|---|---|---|
| Soluble fiber: psyllium, beta-glucan, guar gum, glucomannan | Human outcome evidence, usually modest or mixed | Soluble fiber may support fullness, stool pattern, LDL cholesterol, and calorie control; NIH ODS reports little to no effect on body weight for several fiber ingredients, with product-specific variation.[1] | Does not prove fiber capsules produce large weight loss without broader nutrition changes. | Gas, bloating, constipation, diarrhea, medication-timing issues; glucomannan tablets have obstruction concerns if not taken with enough fluid.[1] |
| Protein powders, meal replacements, collagen, amino acids | Health-behavior and body-composition support | Protein can support satiety and muscle preservation during weight loss, especially with resistance training; meal replacements may help structure intake when used appropriately. | Does not prove more protein automatically causes fat loss or improves health for everyone. | Kidney disease, liver disease, eating disorder history, allergies, and high-calorie “mass gainer” products need caution. |
| Caffeine: coffee extract, guarana, kola nut, yerba maté | Short-term modest or indirect evidence | Caffeine can increase thermogenesis and may have a modest effect on weight or prevention of weight gain in some studies.[1] | Does not prove stimulant products produce durable fat loss. | Jitteriness, insomnia, anxiety, tachycardia, blood-pressure effects, pregnancy limits, and hidden caffeine from multiple ingredients. |
| Green tea and green tea extract | Modest and inconsistent human evidence | Green tea catechins with caffeine may have small effects in some studies; Cochrane-level evidence has not supported meaningful long-term weight loss for most people.[6][9] | Does not prove green tea extract is a safe or powerful fat burner. | Green tea beverage is usually safer; concentrated extracts have been linked to liver injury in some cases.[6] |
| Probiotics, prebiotics, synbiotics | Inconsistent human evidence | NIH ODS describes probiotic effects on body fat, waist, hip circumference, and body weight as inconsistent.[1] | Does not prove “a probiotic” causes weight loss; effects are strain- and product-specific. | Gas and bloating are common; serious infections are rare but possible in severely ill or immunocompromised people.[15] |
| Berberine | Metabolic biomarker evidence; modest weight evidence | Some studies suggest modest effects on weight, BMI, lipids, or glucose markers, but evidence quality and product differences limit confidence. | Does not prove berberine is “natural Ozempic” or comparable to GLP-1 medication. | Can interact with diabetes medicines, anticoagulants, antibiotics, immunosuppressants, pregnancy-related care, and other medications. |
| Chromium | Minimal human weight-loss evidence | NIH ODS describes chromium’s effect on body weight and body fat as minimal.[1] | Does not prove chromium controls cravings or causes fat loss. | Headache, GI symptoms, skin reactions; people with diabetes medication changes should ask a clinician. |
| Vitamin D, magnesium, omega-3s | Deficiency or cardiometabolic context, not weight-loss proof | These nutrients may matter when deficiency or a medical indication exists, but NIH ODS reports no body-weight effect for vitamin D and no general weight-loss role for these as standalone products.[1] | Does not prove correcting a lab value causes weight loss when deficiency is absent. | High-dose vitamin D, magnesium, or omega-3s can be risky in kidney disease, hypercalcemia, arrhythmias, anticoagulant use, or medication-heavy contexts. |
| Apple cider vinegar | Limited and inconsistent human evidence | Some small studies examine satiety, glucose, lipids, or weight, but evidence is not strong enough to call it a reliable weight-loss supplement. | Does not prove vinegar burns fat or replaces nutrition care. | Can worsen reflux, irritate the throat, affect tooth enamel, and interact with diabetes medicines or diuretics. |
| CLA: conjugated linoleic acid | Minimal human weight/body-fat effect | NIH ODS describes CLA’s effect on body weight and body fat as minimal.[1] | Does not prove CLA meaningfully changes body composition for most users. | GI effects and possible adverse effects on blood lipids or glucose homeostasis are concerns.[1] |
| L-carnitine | Possible modest effect, not a fat-burning guarantee | Some meta-analytic evidence suggests modest weight changes, and NIH ODS classifies carnitine as possibly modest for weight reduction.[1][11] | Does not prove carnitine forces fat loss in people with adequate carnitine status. | GI symptoms, fishy body odor, and potential TMAO-related cardiovascular questions.[1] |
| MCT oil and coconut-oil products | Limited or indirect evidence | MCTs may affect satiety or energy expenditure in short studies, but they are still calories and do not reliably cause weight loss. | Does not prove adding oil to the diet reduces body fat. | GI upset and extra calories; coconut oil is not the same as purified MCT oil. |
| Capsaicin and capsaicinoids | Mostly appetite or energy-intake evidence | NIH ODS notes capsaicin might reduce energy intake but reports no effect on body weight.[1] | Does not prove spicy-capsule products cause fat loss. | GI distress, reflux, sweating, and tolerance issues. |
| Garcinia cambogia / hydroxycitric acid | Little to no effect; safety concerns | NIH ODS describes garcinia as having little to no effect on body weight, with safety concerns reported.[1] | Does not prove appetite suppression or fat-blocking claims. | Headache, nausea, GI symptoms, mania reports, liver damage, and serotonin-related medication concerns.[1] |
| White kidney bean, chitosan, green coffee, pyruvate, African mango | Limited, modest, or weak evidence | Some ingredients show possible modest effects in small or methodologically limited trials; NIH ODS emphasizes that more rigorous research is needed for many products.[1] | Does not prove carb-blocker, fat-binder, or metabolism claims translate into meaningful long-term weight loss. | GI symptoms, shellfish allergy for chitosan, caffeine exposure for green coffee, and product-quality concerns. |
| Bitter orange / synephrine | Weak and safety-limited evidence | NIH ODS describes evidence for bitter orange and synephrine as contradictory and weak, with possible effects on metabolic rate but inconclusive weight-loss effects.[1] | Does not prove ephedra-like fat burning is safe or effective. | Chest pain, anxiety, increased heart rate or blood pressure, and serious cardiovascular events have been reported, especially in stimulant combinations.[1] |
| Yohimbe / yohimbine | Safety-concern category | NIH ODS reports no effect on body weight and insufficient evidence for weight loss.[1] | Does not prove fat loss, sexual-performance, or stimulant claims are worth the risk. | Hypertension, tachycardia, anxiety, agitation, heart attack, heart failure, and death have been reported.[1][7] |
| Ashwagandha, adaptogens, cortisol-balancing blends | Indirect stress/sleep evidence, not weight-loss evidence | Some adaptogens have stress or sleep studies, but they are not proven weight-loss supplements. | Does not prove lowering “cortisol” through supplements causes fat loss. | Ashwagandha should be avoided in pregnancy and has been linked to rare liver-injury reports.[16] |
| Detox teas, laxatives, diuretics, “cleanse” products | Safety concern, not fat-loss evidence | These products may reduce scale weight through water loss or stool changes, not fat loss. | Does not prove detoxification, metabolic reset, or sustained weight loss. | Dehydration, electrolyte imbalance, diarrhea, kidney strain, laxative dependence, and medication interactions. |
| Ephedra, DMAA, hidden-drug products, illegal stimulants | Avoid / safety concern | Ephedra-containing dietary supplements were banned in the United States because of unreasonable risk, and FDA warns many weight-loss products contain dangerous hidden ingredients.[5][8] | Does not prove “stronger stimulant” means safer or better fat loss. | Serious cardiovascular, neurologic, psychiatric, and hospitalization risks. |
Supplement-by-Supplement Evidence
Soluble Fiber: Psyllium, Glucomannan, Beta-Glucan, and Guar Gum
Fiber is one of the more sensible supplement categories because it can support fullness, stool regularity, LDL cholesterol, and glucose response in some people. But the weight-loss evidence is still modest. NIH ODS reports that beta-glucans and guar gum generally do not have a significant effect on weight loss, while glucomannan shows little to no effect on body weight in clinical trials of varying quality.[1]
Psyllium is often more useful as a stool-pattern and cholesterol-support fiber than as a direct weight-loss product. Glucomannan deserves special caution because tablet forms may swell and cause esophageal obstruction if taken without enough fluid, while powders and capsules can cause gas, bloating, diarrhea, constipation, or abdominal discomfort.[1] Fiber can also affect medication absorption, so timing matters for people taking thyroid medication, diabetes medication, iron, antidepressants, or other daily prescriptions.
Protein Powders, Meal Replacements, Collagen, and Amino Acids
Protein is relevant to weight management because it can support satiety and help preserve lean mass during weight loss, especially when combined with resistance training. But protein powders are not fat-loss drugs. A shake can help if it replaces a higher-calorie meal in a structured plan; it can also prevent weight loss if it simply adds extra calories on top of usual intake.
Collagen is not a complete protein source in the same way whey, soy, pea, egg, or mixed complete proteins can be, because it is low in some essential amino acids. Essential amino acid and BCAA products are often marketed for muscle, but they do not replace a complete diet or resistance training. People with kidney disease, liver disease, dialysis status, cancer cachexia, eating disorder history, or very low appetite should ask for individualized nutrition guidance rather than following a generic high-protein plan.
Caffeine and Herbal Caffeine Sources
Caffeine can temporarily increase energy expenditure, alertness, and fat oxidation, which is why it appears in many weight-loss supplements. NIH ODS describes caffeine as possibly having a modest effect on body weight or reduced weight gain over time, but much of the evidence comes from short-term studies or multi-ingredient products.[1]
The safety issue is dose stacking. A label may list guarana, yerba maté, kola nut, green tea, coffee extract, and “energy blend” without making the total caffeine obvious. Too much caffeine can cause jitteriness, anxiety, insomnia, vomiting, tremor, tachycardia, palpitations, and blood-pressure effects.[1] People with panic disorder, arrhythmias, uncontrolled hypertension, pregnancy, insomnia, stimulant prescriptions, or heavy caffeine use should be especially cautious.
Green Tea and Green Tea Extract
Green tea beverage and concentrated green tea extract should not be treated as the same product. Green tea contains catechins and caffeine, and some studies show small effects on energy expenditure or body weight. However, Cochrane review evidence does not support meaningful weight loss or weight maintenance effects for most adults with overweight or obesity.[9]
Safety is the stronger reason to be cautious. NCCIH notes that green tea beverages are generally safe for most people, but green tea extract has been linked to liver problems in rare cases.[6] NIH ODS also lists constipation, abdominal discomfort, nausea, increased blood pressure, and liver damage as reported adverse effects for green tea extract.[1] A capsule with high EGCG content is not the same as drinking brewed tea.
Probiotics, Prebiotics, and Synbiotics
The gut microbiome is involved in energy harvest, appetite signaling, inflammation, bile acids, and glucose metabolism, so probiotic weight-loss claims are biologically plausible. But “probiotics” are not one intervention. Effects depend on strain, dose, duration, diet, baseline microbiome, and the outcome measured.
NIH ODS describes probiotic effects on body fat, waist and hip circumference, and body weight as inconsistent.[1] NCCIH notes that probiotics are generally well tolerated by many healthy people, but serious infections have occurred in high-risk people, including those who are severely ill or immunocompromised.[15] A probiotic should not be chosen by strain count alone, and “more CFUs” does not automatically mean better weight outcomes.
Berberine
Berberine is often marketed as “nature’s Ozempic,” but that comparison is misleading. Berberine is not a GLP-1 receptor agonist, does not have the same mechanism as semaglutide or tirzepatide, and is not an FDA-approved weight-loss medication. Some studies suggest modest changes in body weight, BMI, glucose, LDL cholesterol, triglycerides, or inflammation, but evidence quality varies and many trials are small or have bias concerns.
The safety profile is more drug-like than many supplement ads suggest. Berberine may interact with diabetes medications, blood thinners, antibiotics, immunosuppressants, blood-pressure medications, and pregnancy-related care. It can also cause constipation, diarrhea, gas, nausea, or abdominal discomfort. It should not be used as a substitute for prescribed diabetes or weight-management care.
Chromium
Chromium is marketed for cravings, blood sugar, and fat loss. NIH ODS describes the weight-related evidence as minimal for body weight and body fat.[1] That makes chromium a weak choice for weight loss unless there is a specific clinician-guided reason to discuss it.
People taking diabetes medications should be cautious because any supplement that claims to affect glucose may complicate blood-sugar management. Reported adverse effects include headache, watery stools, constipation, weakness, vertigo, nausea, vomiting, and hives.[1]
Vitamin D, Magnesium, Omega-3s, and “Deficiency Correction” Supplements
Vitamin D, magnesium, and omega-3s may be important for health in the right context, but they should not be framed as weight-loss supplements for everyone. NIH ODS reports that vitamin D has no effect on body weight in clinical trials, despite associations between low vitamin D status and obesity.[1] Low vitamin D can be a consequence or correlate of other factors rather than a direct cause of weight gain.
Magnesium may be useful when intake is low or deficiency exists, but high-dose supplemental magnesium can cause diarrhea and may accumulate in kidney disease.[17] Omega-3s may be relevant for triglycerides or cardiovascular-risk discussions, but fish oil is not a weight-loss supplement. Deficiency correction is legitimate medicine; using deficiency language to sell general fat-loss products is not.
Apple Cider Vinegar
Apple cider vinegar is marketed for appetite, glucose response, and fat loss, but the human evidence is limited and inconsistent. Any possible effect is likely related to short-term satiety, slowed gastric emptying, or changes in meal pattern—not direct fat burning. A tablespoon of vinegar is not comparable to a prescription weight-loss medication, and dramatic claims should be treated skeptically.
Safety is mostly about acidity and medication context. Vinegar can irritate the throat or stomach, worsen reflux, contribute to tooth enamel erosion, and affect blood sugar in people taking diabetes medications. People with gastroparesis, significant reflux, ulcers, kidney disease, low potassium, diuretic use, insulin use, or pregnancy should ask a clinician before using it regularly.
CLA: Conjugated Linoleic Acid
CLA has been studied for body composition and fat metabolism, but the average effect is small. NIH ODS describes CLA as having a minimal effect on body weight and body fat.[1] It should not be presented as a reliable way to “cut fat” or preserve muscle.
Possible side effects include abdominal discomfort, constipation, diarrhea, loose stools, dyspepsia, and concerns about adverse effects on blood lipids or glucose homeostasis.[1] People with diabetes, metabolic syndrome, liver disease, or lipid disorders should be cautious.
L-Carnitine
L-carnitine participates in fatty-acid transport into mitochondria, which makes it easy to market as a fat-burning supplement. Human results are more modest. NIH ODS classifies carnitine as possibly producing modest weight reduction, while noting adverse effects and uncertainty about TMAO, a metabolite linked with cardiovascular risk markers.[1] A meta-analysis of randomized trials also reported weight-related effects, but that does not make carnitine a guaranteed fat-loss product.[11]
Side effects can include nausea, vomiting, diarrhea, abdominal cramps, and fishy body odor.[1] It may be more relevant in certain deficiency or medical contexts than as a general weight-loss aid.
MCT Oil
MCT oil is calorie-containing fat, not a calorie-free metabolism booster. Some short-term studies suggest medium-chain triglycerides may affect satiety or energy expenditure differently than long-chain fats, but adding oil to the diet can easily increase total calories. Any benefit depends on replacing other calories, not simply adding MCT oil to coffee, smoothies, or meals.
Common side effects include diarrhea, cramping, nausea, and urgent stools. People with liver disease, pancreatitis history, gallbladder issues, reflux, or very high triglycerides should discuss use with a clinician. Coconut oil is not the same as purified MCT oil and should not be marketed as equivalent.
Capsaicin, Capsicum, and “Thermogenic” Pepper Extracts
Capsaicin and related capsaicinoids may increase thermogenesis slightly and may reduce energy intake in some studies. NIH ODS notes that capsaicin might reduce energy intake but has no effect on body weight.[1] That means spicy supplements may influence appetite or heat sensation without translating into meaningful fat loss.
Side effects include reflux, stomach discomfort, sweating, flushing, and diarrhea. People with GERD, ulcers, irritable bowel symptoms, hemorrhoids, or medication sensitivity may tolerate food-based spices better than concentrated capsules.
Garcinia Cambogia
Garcinia cambogia contains hydroxycitric acid, often marketed as an appetite suppressant or fat-synthesis blocker. NIH ODS describes its weight effect as little to no effect, and a systematic review found that any short-term weight effect was small and uncertain.[1][10]
The safety cautions are important. NIH ODS lists headache, nausea, respiratory symptoms, gastrointestinal symptoms, mania, and liver damage among reported adverse effects.[1] Garcinia products may also be risky with serotonergic medications, bipolar disorder, liver disease, alcohol-related liver risk, or multi-ingredient fat-burner formulas.
White Kidney Bean, Chitosan, Green Coffee, Pyruvate, and African Mango
These products are often marketed as carb blockers, fat binders, metabolism boosters, or appetite products. NIH ODS summarizes several as having possible modest effects, minimal effects, or insufficient research because studies are small, short, poorly controlled, or based on combination products.[1]
Chitosan may trigger shellfish-allergy concerns and can cause bloating, constipation, indigestion, nausea, or heartburn.[1] Green coffee contains caffeine-like compounds and may cause headache or urinary symptoms. White kidney bean extract may cause flatulence, soft stools, or constipation. These products should not be used to justify eating patterns that otherwise worsen glucose, reflux, or GI symptoms.
Bitter Orange, Synephrine, and Stimulant Fat Burners
Bitter orange became common after ephedra was banned from dietary supplements in the United States. It is usually marketed as a thermogenic stimulant, often combined with caffeine. NIH ODS states that evidence for bitter orange or synephrine is contradictory and weak, and that safety concerns have been reported, especially in stimulant combinations.[1]
Reported adverse events include chest pain, headache, anxiety, elevated heart rate, ventricular fibrillation, ischemic stroke, myocardial infarction, and death, although many products involved multiple ingredients and causality can be difficult to isolate.[1] People with high blood pressure, arrhythmias, panic disorder, insomnia, stimulant prescriptions, or heavy caffeine use should avoid stimulant stacking unless a clinician has reviewed it.
Yohimbe and Yohimbine
Yohimbe is sometimes included in weight-loss, energy, and sexual-performance products. NIH ODS reports no effect on body weight and insufficient evidence for weight loss.[1] NCCIH also emphasizes safety concerns and notes that yohimbe products have been associated with serious adverse effects.[7]
This is one of the clearest “avoid or use only with medical guidance” categories. NIH ODS lists headache, anxiety, agitation, hypertension, tachycardia, myocardial infarction, cardiac failure, and death among reported adverse effects.[1] It is especially risky with blood-pressure medications, stimulants, antidepressants, anxiety disorders, heart disease, and psychiatric medications.
Ashwagandha, Adaptogens, and Cortisol-Marketed Products
Ashwagandha, rhodiola, ginseng, saffron, and other botanicals may have stress, fatigue, or sleep-related studies, but they are not proven weight-loss supplements. Weight gain can be influenced by sleep and stress, but it does not follow that taking an adaptogen causes fat loss.
Ashwagandha is a good example of why “natural” does not mean risk-free. NCCIH notes that ashwagandha should be avoided during pregnancy and has been linked to rare liver-injury reports.[16] Botanicals can also interact with sedatives, thyroid medications, immunosuppressants, diabetes medicines, blood thinners, and psychiatric medications.
Detox Teas, Laxatives, Diuretics, and Cleanse Products
Detox teas and cleanse products may reduce scale weight through water loss or stool changes, not fat loss. A lower morning weight after diarrhea, sweating, or diuresis is not the same as sustained body-fat reduction. These products can also reinforce unsafe weight-control behaviors in people vulnerable to eating disorders.
Safety risks include dehydration, low potassium, dizziness, fainting, diarrhea, cramps, kidney strain, laxative dependence, and interactions with diuretics, heart medications, lithium, blood-pressure medications, and diabetes medications. Products that promise “rapid detox weight loss” should be treated as high-risk marketing.
Ephedra, DMAA, Hidden-Drug Products, and Adulterated Fat Burners
Ephedra is no longer allowed in dietary supplements in the United States because FDA determined that ephedrine alkaloids present an unreasonable risk of illness or injury.[8] FDA also warns that many weight-loss products marketed as dietary supplements, teas, pills, or “all natural” products are likely to be contaminated with dangerous hidden ingredients and can lead to hospitalization.[5]
The FDA weight-loss product notification database repeatedly lists products found to contain hidden drug ingredients, and FDA warns that the list covers only a fraction of contaminated products on the market.[5] Products sold online, through social media, or with extreme claims such as “works like prescription medication,” “no diet needed,” or “lose 20 pounds fast” deserve special skepticism.
Prescription and Drug-Like Weight-Loss Options Are Not Supplements
Orlistat, GLP-1 medications, phentermine/topiramate, naltrexone/bupropion, metformin, and bariatric procedures belong in medical care, not supplement shopping. Orlistat has an over-the-counter lower-dose version, but it is still a drug, not a dietary supplement. GLP-1 medications and related incretin therapies require diagnosis, contraindication review, prescription access, side-effect planning, and follow-up.
NIDDK notes that prescription weight-management medications may be used when lifestyle changes are not enough and that patients should discuss health issues, other medications, family history, cost, and side effects with a health professional.[4] Supplements should not be used as substitutes for evidence-based obesity treatment, diabetes care, sleep apnea treatment, or bariatric evaluation when those are medically appropriate.
Safety, Interactions, and Who Should Be Careful
Weight-loss supplements are often taken by people who are also using medications, restricting food, increasing exercise, or managing chronic health conditions. That is exactly when risk can increase. The table below highlights common caution zones.
| Situation | Supplements to review first | Why it matters |
|---|---|---|
| Heart disease, arrhythmias, palpitations, high blood pressure, panic disorder, or insomnia | Caffeine, guarana, bitter orange, yohimbe, synephrine, “thermogenic” blends, pre-workouts, hidden-drug products. | Stimulants can raise heart rate, blood pressure, anxiety, insomnia, and rhythm risk in susceptible people.[1] |
| Liver disease, heavy alcohol use, elevated liver enzymes, or jaundice history | Green tea extract, garcinia, ashwagandha, kava, multi-herb fat burners, high-dose niacin, unknown blends. | Some concentrated botanical products have been linked with liver injury, and multi-ingredient blends are hard to evaluate.[6][16] |
| Diabetes, glucose-lowering medications, or hypoglycemia risk | Berberine, chromium, apple cider vinegar, cinnamon blends, bitter melon, alpha-lipoic acid, stimulant products. | Blood sugar may change, medication effects may become harder to predict, and symptoms can be masked by stimulants. |
| Eating disorder history, laxative misuse, extreme restriction, or body-image distress | Detox teas, laxatives, appetite suppressants, stimulant fat burners, scale-focused products. | These products can reinforce unsafe behaviors and can worsen electrolyte, heart rhythm, mood, and nutrition risk. |
| Pregnancy, trying to conceive, or breastfeeding | Most weight-loss supplements, stimulants, detox products, berberine, ashwagandha, high-dose caffeine, unknown botanicals. | Weight-loss supplementation is often inappropriate, and safety data may be limited. Pregnancy-related weight concerns need clinical care. |
| Kidney disease, kidney stones, dehydration risk, or diuretic use | Protein powders, creatine, magnesium, potassium electrolytes, detox teas, laxatives, apple cider vinegar, high-dose vitamin C. | Kidney function, hydration, potassium, magnesium, acid-base balance, and stone risk can change supplement safety. |
| Psychiatric medications, bipolar disorder, anxiety disorder, seizures, or antidepressant use | Stimulants, yohimbe, garcinia, 5-HTP, St. John’s wort, berberine, “mood and appetite” blends. | Serotonin, stimulant, sleep, seizure-threshold, and mood-cycling effects may matter clinically. |
| Anticoagulants, antiplatelets, bleeding disorder, or upcoming surgery | Fish oil, turmeric/curcumin, garlic, ginkgo, green tea extract, berberine, multi-herb blends. | Bleeding risk, anesthesia planning, and drug metabolism should be reviewed in advance. |
| Adolescents or young adults | Stimulants, detox teas, appetite suppressants, body-composition stacks, “fat burners.” | Growth, mental health, eating-disorder risk, sports pressures, and hidden stimulant exposure deserve special caution. |
What the Research Does Not Prove
The research does not prove that weight-loss supplements can override calorie intake, sleep loss, alcohol intake, medication-induced weight gain, untreated sleep apnea, chronic stress, binge eating, endocrine disorders, or limited access to safe food and activity. It also does not prove that a supplement that changes a biomarker—such as glucose, insulin, thermogenesis, gut bacteria, or fat oxidation—causes meaningful fat loss.
The research does not prove that multi-ingredient products are better than single ingredients. In fact, NIH ODS notes that multi-ingredient products make it difficult to isolate the effects of individual ingredients and predict the effects of combinations.[1] A product may contain caffeine, synephrine, green tea extract, yohimbine, diuretics, laxatives, and undisclosed substances, making the risk much higher than the evidence suggests for any one ingredient.
The research also does not prove that “natural” products are safer than prescription medications. FDA does not approve dietary supplements for safety and effectiveness before marketing in the same way it approves drugs, and manufacturers are responsible for ensuring that their products meet safety standards and labeling requirements.[2]
How to Talk to a Clinician About Supplements
A useful clinician conversation starts with the goal. “I want to lose weight” can mean many things: lowering A1C, reducing blood pressure, improving mobility, preparing for surgery, reducing sleep apnea symptoms, changing body composition, improving cholesterol, or addressing weight gain from a medication. The safer supplement discussion depends on that goal.
Useful questions include:
- Is weight loss medically appropriate for me right now?
- Could my weight change be related to medication, sleep apnea, thyroid disease, depression, menopause, PCOS, pain, stress, or another condition?
- Does this supplement have human weight-loss evidence, or only appetite, glucose, thermogenesis, animal, or mechanism evidence?
- Could it interact with my medications, including diabetes medicines, blood-pressure medicines, antidepressants, stimulants, anticoagulants, or hormone therapy?
- Does my liver, kidney, heart, blood-pressure, pregnancy, or eating-disorder history make this product risky?
- What should I track besides scale weight: waist, strength, energy, sleep, blood pressure, glucose, symptoms, or labs?
- What symptom or side effect should make me stop and call?
How to Choose Supplements More Safely
Safer supplement selection starts with avoiding extreme claims. Be skeptical of products that promise “rapid fat melting,” “works like Ozempic,” “no diet needed,” “detox weight loss,” “hormone reset,” “guaranteed results,” or “clinical strength” without naming the actual study, dose, population, and outcome. FDA warns that many weight-loss products marketed as supplements may contain hidden drug ingredients and that absence from FDA’s list does not prove a product is safe.[5]
Look for transparent ingredient amounts, no proprietary stimulant blends, a full Supplement Facts label, lot number, expiration date, allergen information, and third-party testing when available. Third-party testing does not prove weight-loss benefit, but it can help reduce some identity and contamination concerns. Avoid starting multiple products at once; if a side effect or lab change occurs, a stack makes it hard to identify the cause.
Also check the calorie context. Protein powders, MCT oil, collagen drinks, “keto coffee,” gummies, bars, and meal-replacement shakes can add calories. A product that helps one person reduce total intake can cause another person to gain weight if it is simply added to the diet.
Common Mistakes to Avoid
- Expecting supplement-level effects from medication-level marketing. Most supplements produce small or uncertain average effects, if any.
- Confusing water loss with fat loss. Diuretics, laxatives, sweating, and dehydration can lower scale weight without reducing fat.
- Stacking stimulants. Caffeine plus guarana, green tea extract, synephrine, yohimbine, and pre-workout products can increase heart and anxiety risks.
- Ignoring liver symptoms. Jaundice, dark urine, severe fatigue, nausea, or right-upper-abdominal pain after starting a supplement should be evaluated.
- Using supplements to compensate for disordered eating. Appetite suppression, laxatives, detox teas, or compulsive tracking can worsen eating-disorder risk.
- Assuming all “natural” products are safe. FDA warns that many weight-loss products marketed as natural can contain hidden ingredients.[5]
- Not telling clinicians about supplements. Supplements can matter for blood pressure, glucose, liver enzymes, kidney labs, surgery, and drug interactions.
- Buying from social media urgency claims. “Limited-time,” “secret doctor formula,” and “banned ingredient” marketing are warning signs.
FAQ
Do weight-loss supplements actually work?
Some have modest evidence, but no supplement reliably produces large, durable weight loss for most people. Effects are usually small and depend on the full weight-management plan.[1]
What is the safest weight-loss supplement?
There is no universally safest option. Plain soluble fiber or protein support may be reasonable for some people, but safety depends on GI tolerance, medications, kidney function, allergies, and eating patterns.
Is green tea extract good for weight loss?
Green tea extract may have small effects in some studies, but meaningful long-term weight loss is not well supported. Concentrated extracts can also carry liver-safety concerns.[6][9]
Is berberine the same as Ozempic?
No. Berberine is not a GLP-1 medication and should not be described as natural Ozempic. It may affect metabolic markers, but it is not equivalent to prescription incretin therapy.
Are detox teas useful for fat loss?
No. Detox teas usually affect water loss, stool output, or GI irritation rather than body fat. They can cause dehydration, diarrhea, electrolyte imbalance, and laxative misuse risk.
What ingredients should be avoided?
Use strong caution with yohimbe, bitter orange plus caffeine, stimulant fat burners, detox/laxative products, hidden-drug products, ephedra-like ingredients, and products promising rapid results.[5][7][8]
Sources and Evidence Method
This article prioritized human randomized trials, systematic reviews, government supplement-safety resources, and clinical guidance relevant to weight management. Evidence was classified as human weight-loss evidence when studies measured weight, BMI, waist circumference, body fat, or weight maintenance; modest or indirect evidence when studies measured appetite, thermogenesis, glucose, lipids, fat oxidation, microbiome changes, or short-term intake; limited/no evidence when claims depended mainly on mechanism or small studies; and safety concern when a product is common in weight-loss marketing but has meaningful adverse-event or adulteration risk.
The article avoids affiliate-style product rankings because supplement effects depend on dose, formulation, baseline diet, medical history, medication use, sleep, activity, and product quality. A trial of one branded extract, one dose, or one population should not be generalized to every product in a category.
Author, Reviewer, and Last Updated
References
- National Institutes of Health Office of Dietary Supplements. (n.d.). Dietary supplements for weight loss: Fact sheet for health professionals.
- U.S. Food and Drug Administration. (2024). Questions and answers on dietary supplements.
- U.S. Preventive Services Task Force. (2018). Weight loss to prevent obesity-related morbidity and mortality in adults: Behavioral interventions.
- National Institute of Diabetes and Digestive and Kidney Diseases. (n.d.). Prescription medications to treat overweight and obesity. National Institutes of Health.
- U.S. Food and Drug Administration. (2026). Weight loss product notifications.
- National Center for Complementary and Integrative Health. (n.d.). Green tea: Usefulness and safety. National Institutes of Health.
- National Center for Complementary and Integrative Health. (n.d.). Yohimbe: Usefulness and safety. National Institutes of Health.
- National Center for Complementary and Integrative Health. (n.d.). Ephedra: Usefulness and safety. National Institutes of Health.
- Jurgens, T. M., Whelan, A. M., Killian, L., Doucette, S., Kirk, S., & Foy, E. (2012). Green tea for weight loss and weight maintenance in overweight or obese adults. Cochrane Database of Systematic Reviews, 12, CD008650.
- Onakpoya, I., Hung, S. K., Perry, R., Wider, B., & Ernst, E. (2011). The use of Garcinia extract (hydroxycitric acid) as a weight loss supplement: A systematic review and meta-analysis of randomised clinical trials. Journal of Obesity, 2011, 509038.
- Pooyandjoo, M., Nouhi, M., Shab-Bidar, S., Djafarian, K., & Olyaeemanesh, A. (2016). The effect of L-carnitine on weight loss in adults: A systematic review and meta-analysis of randomized controlled trials. Obesity Reviews, 17(10), 970–976.
- Kreider, R. B., Kalman, D. S., Antonio, J., Ziegenfuss, T. N., Wildman, R., Collins, R., Candow, D. G., Kleiner, S. M., Almada, A. L., & Lopez, H. L. (2017). International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14, 18.
- Reynolds, A., Mann, J., Cummings, J., Winter, N., Mete, E., & Te Morenga, L. (2019). Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. The Lancet, 393(10170), 434–445.
- National Institutes of Health Office of Dietary Supplements. (2024). Omega-3 fatty acids: Fact sheet for health professionals.
- National Center for Complementary and Integrative Health. (2025). Probiotics: Usefulness and safety. National Institutes of Health.
- National Center for Complementary and Integrative Health. (2024). Ashwagandha: Usefulness and safety. National Institutes of Health.
- National Institutes of Health Office of Dietary Supplements. (2022). Magnesium: Fact sheet for health professionals.