
Quick Answer: Peppermint Oil vs Psyllium vs Probiotics for IBS
For IBS, peppermint oil, psyllium, and probiotics are not competing versions of the same thing. Enteric-coated peppermint oil is best supported for short-term relief of abdominal pain, cramping, and some global IBS symptoms. Psyllium is a soluble, gel-forming fiber that is most relevant when stool form is part of the problem, especially in IBS-C and mixed bowel patterns. Probiotics are popular and biologically plausible, but guideline recommendations are cautious because trial results vary widely by strain, dose, study design, and symptom target.[1][2]
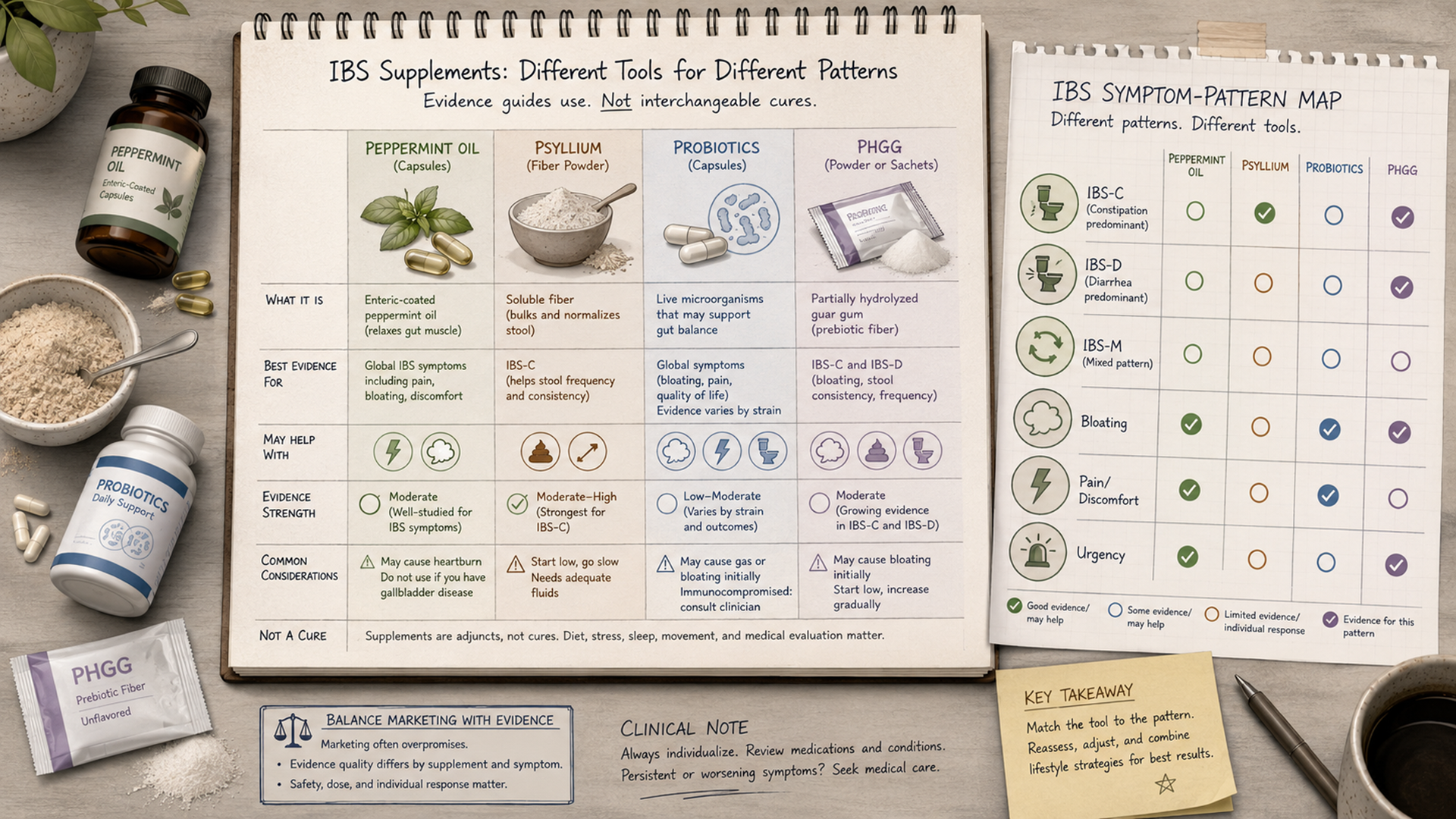
The most practical comparison is by symptom pattern. IBS-C usually points first toward soluble fiber options such as psyllium, with PHGG as a possible gentler fiber alternative for some people. IBS-D may involve pain, urgency, and loose stool, so peppermint oil may be more relevant for cramping while small, carefully tolerated amounts of soluble fiber may help stool form. IBS-M often needs a slower, more cautious approach because constipation and diarrhea alternate. Bloating can improve or worsen with any supplement, depending on the product and the person.[1][4]
No supplement confirms an IBS diagnosis, replaces a clinician’s evaluation, or works for everyone. IBS is now classified as a disorder of gut-brain interaction, meaning symptoms can reflect bowel sensitivity, motility changes, immune signaling, microbiome changes, stress-system signaling, and food-triggered fermentation rather than one single cause.[3] That is why a subtype-based, symptom-based approach is more useful than asking for one “best supplement for IBS.”
Professional-care note: this article is educational and does not diagnose IBS or tell any reader which supplement to use. New, severe, worsening, or unusual digestive symptoms should be evaluated by a qualified clinician, especially when red flags such as bleeding, anemia, unexplained weight loss, fever, nighttime diarrhea, or a family history of colorectal cancer, inflammatory bowel disease, or celiac disease are present.
Best Supplement by IBS Type and Symptom Pattern
The table below summarizes how peppermint oil, psyllium, probiotics, and PHGG generally fit different IBS patterns. It is not a treatment plan. It is a way to interpret the evidence without turning supplement marketing into medical advice.
| IBS pattern or symptom | Most relevant option | Why it may fit | Main caution |
|---|---|---|---|
| IBS-C: constipation-predominant IBS | Psyllium; PHGG may be considered as another soluble fiber option. | Soluble fiber can help improve stool form and bowel regularity. Guidelines generally favor soluble fiber over insoluble fiber such as wheat bran for IBS symptoms.[1][8] | Fiber can worsen gas, bloating, or cramping if increased too fast or if the product contains poorly tolerated additives. |
| IBS-D: diarrhea-predominant IBS | Peppermint oil for cramping; psyllium may help stool form in some cases. | Peppermint oil has antispasmodic effects and has been studied for global IBS symptoms and abdominal pain. Psyllium’s gel-forming properties may help some people with loose stool consistency.[4][5] | Persistent diarrhea, dehydration, blood in stool, fever, or nighttime diarrhea needs medical assessment rather than supplement trial-and-error. |
| IBS-M: mixed constipation and diarrhea | Psyllium or PHGG may be more logical than a strongly laxative or strongly constipating product. | A gentle soluble fiber strategy may be useful when stool pattern swings between hard and loose stools, but tolerance matters more than the label claim. | Changing several supplements at once makes it difficult to know what helped or what caused a flare. |
| Pain and cramping | Enteric-coated peppermint oil. | Peppermint oil relaxes intestinal smooth muscle, and meta-analyses suggest benefit for abdominal pain and global IBS symptoms, though evidence quality and trial heterogeneity remain limitations.[4][5] | It can worsen reflux, heartburn, indigestion, nausea, or perianal burning, especially if capsules are not enteric coated or are taken with acid-suppressing products that affect coating behavior.[10] |
| Bloating and gas | Peppermint oil may help crampy bloating; low-FODMAP evaluation may matter more than supplements. | Bloating can come from bowel sensitivity, gas handling, constipation, FODMAP fermentation, and gut-brain signaling, so one supplement rarely solves every driver.[2] | Probiotics, fibers, inulin, sugar alcohols, and prebiotic blends can worsen gas in some people. |
| Urgency and loose stool | Psyllium may help stool consistency; peppermint oil may help if urgency is tied to cramping. | Soluble fiber can hold water and form a gel, which may improve stool form. Peppermint oil targets spasmodic pain rather than the underlying cause of diarrhea. | Frequent urgency with weight loss, bleeding, fever, anemia, or new onset later in life should not be managed as routine IBS without evaluation. |
| “Microbiome support” as the main goal | Probiotics only when strain-specific rationale and safety make sense. | Some trials report symptom improvement with certain probiotics, but results are inconsistent and cannot be generalized from one strain or blend to another.[6][7] | People who are immunocompromised, critically ill, have central venous catheters, or have complex medical conditions should not treat probiotics as automatically safe.[11] |
First: Make Sure It Is Really IBS
IBS is usually defined by recurring abdominal pain associated with changes in bowel habits, such as constipation, diarrhea, or both. The diagnosis is clinical, meaning it depends on symptom pattern, history, exam findings, and selective testing rather than one single blood test or scan. Current guidelines emphasize making a positive diagnosis when the pattern fits, while still checking for alarm features that suggest another condition.[1][9]
This matters because “IBS-like” symptoms can also occur with celiac disease, inflammatory bowel disease, microscopic colitis, bile acid diarrhea, lactose intolerance, medication side effects, infections, endometriosis, thyroid disease, and colorectal cancer. Supplements can temporarily change symptoms and make the pattern harder to interpret. They should not be used to delay evaluation when symptoms are new, progressive, severe, or different from a person’s usual pattern.
Peppermint Oil for IBS: Best Fit for Pain, Cramping, and Short-Term Global Symptoms
Peppermint oil is the best-known supplement option for IBS pain and cramping. Its main active component, menthol, can relax intestinal smooth muscle by affecting calcium channels, which is why it is often described as an antispasmodic. In IBS, this mechanism is most relevant when symptoms feel like cramping, spasms, pressure, or pain that comes with bowel activity rather than when the main issue is hard stool or frequent watery stool.[5]
Evidence reviews generally find that peppermint oil performs better than placebo for global IBS symptoms and abdominal pain, but the certainty is not perfect. Studies differ in formulation, dose, duration, diagnostic criteria, and outcome measures. The strongest commercial takeaway is not “any peppermint works.” It is that most IBS trials use enteric-coated peppermint oil capsules, designed to release the oil in the intestine rather than the stomach.[4][5]
Peppermint tea and peppermint-flavored foods are not equivalent to studied enteric-coated capsules. Peppermint essential oil should not be treated as a casual oral supplement. Peppermint oil can cause heartburn, reflux, indigestion, nausea, allergic reactions, and burning around the anus; it may be poorly suited for people with significant reflux or certain upper-GI conditions. Pregnancy, breastfeeding, childhood use, gallbladder disease, liver disease, and medication interactions deserve clinician or pharmacist input before use.[10]
Psyllium for IBS: Best Fit for Stool Form in IBS-C and IBS-M
Psyllium is a soluble, gel-forming fiber from Plantago ovata husk. In plain English, it absorbs water and forms a soft gel in the gut. That makes it different from stimulant laxatives, magnesium products, or insoluble wheat bran. For IBS, guidelines and reviews generally favor soluble fiber such as psyllium over insoluble fiber, which may worsen pain, bloating, or stool urgency in some people.[1][4][8]
Psyllium is most relevant for IBS-C, where constipation and hard stools dominate, and IBS-M, where stool form swings between hard and loose. It may also help some people with IBS-D by improving stool consistency, but it should not be framed as a cure for diarrhea. If the main symptoms are watery diarrhea, fever, bleeding, dehydration, or nighttime bowel movements, the priority is clinical assessment rather than adding fiber.
The main limitation is tolerance. Psyllium can cause gas, bloating, fullness, and cramping, especially when introduced quickly or taken without enough fluid. It can also affect absorption of some medications, so spacing from medicines is often recommended on product labels and drug-information resources. Products that combine psyllium with inulin, sugar alcohols, stimulant laxatives, or large sweetener loads may be harder to interpret because the reaction may come from the add-on ingredients rather than the psyllium itself.[12]
Probiotics for IBS: Popular, Plausible, but Less Predictable
Probiotics are live microorganisms intended to provide a health benefit when consumed in adequate amounts. IBS has a plausible microbiome angle: some people develop IBS after infection, symptoms can overlap with fermentation and gas sensitivity, and gut bacteria interact with immune and gut-brain signaling. Plausible biology, however, is not the same as reliable product guidance.[3][6]
The problem is that “probiotics” is not one intervention. A single-strain Bifidobacterium product, a Lactobacillus blend, a Saccharomyces boulardii yeast product, and a 20-strain proprietary blend are scientifically different. Trials vary by strain, dose, duration, population, and symptom target. That is why some reviews find possible benefit in certain analyses while major guidelines remain cautious or recommend against routine probiotic use for global IBS symptoms because the evidence does not translate cleanly into a dependable “best probiotic for IBS-C” or “best probiotic for IBS-D” recommendation.[6][7]
For commercial comparison, probiotics should be judged by strain-level transparency, trial relevance, safety, storage requirements, and whether the company lists viable CFU count through expiration rather than only at manufacturing. More strains and higher CFU counts do not automatically mean better IBS results. Probiotics can cause gas and bloating, and rare serious infections have been reported in higher-risk groups such as severely ill or immunocompromised patients.[11]
Where PHGG Fits: A Gentler Fiber Option for Some People
PHGG stands for partially hydrolyzed guar gum. It is a soluble fiber made by breaking guar gum into smaller, more water-soluble fragments. PHGG is often marketed as a gentler fiber because it dissolves easily and is usually less thick than psyllium. Small clinical studies suggest PHGG may improve IBS symptoms and quality-of-life measures in some patients, but the evidence base is smaller than the evidence base behind psyllium and peppermint oil.[13]
PHGG may be most relevant when a person wants a soluble fiber option but does not tolerate psyllium’s texture, thickness, or bloating. It may also be attractive to people following a low-FODMAP approach if the specific product is certified or otherwise clearly compatible with that plan. The key caution is the same as with other fibers: fiber is not automatically gentle for every IBS pattern, and symptoms can worsen if fermentation, gas sensitivity, constipation, or product additives are not considered.
What to Look For Before Buying IBS Supplements
For IBS supplements, product selection matters because the label category often tells less than the ingredient list, formulation, and evidence target. A peppermint product may be useful or irritating depending on whether it is enteric coated. A fiber product may be psyllium, PHGG, methylcellulose, inulin, wheat dextrin, or a blend. A probiotic may list exact strains or hide behind a broad “proprietary blend.”
| Category | What to look for | What to avoid or question | Best-fit use case |
|---|---|---|---|
| Peppermint oil | Enteric-coated capsules, clear peppermint oil amount, clear serving instructions, allergen information, third-party testing where available. | Essential oil meant for aromatherapy, vague “digestive blend” products, non-enteric liquids for IBS claims, or products that do not list active amounts. | Pain, cramping, spasms, and short-term global IBS symptom support. |
| Psyllium | Plain psyllium husk powder or capsules, minimal additives, clear fiber amount per serving, instructions to take with fluid. | Blends with inulin, sugar alcohols, stimulant laxatives, large sweetener loads, or unclear fiber type. | IBS-C, IBS-M, and stool consistency support. |
| PHGG | Product clearly labeled “partially hydrolyzed guar gum,” good dissolvability, minimal additives, low-FODMAP certification if relevant. | Regular guar gum products marketed as the same thing, proprietary fiber blends, or products with added fermentable fibers that may drive gas. | A soluble fiber alternative when psyllium is not tolerated or texture is a problem. |
| Probiotics | Full strain names, CFU count through expiration, storage instructions, trial references that match the strain, third-party testing where available. | “More strains is better” marketing, undisclosed blends, vague microbiome claims, or products promising to cure IBS. | Selective, strain-specific trials rather than broad first-line IBS use. |
| Low-FODMAP resources | Dietitian-led or evidence-based resources that explain elimination, reintroduction, and personalization phases. | Permanent restriction plans, fear-based food lists, or programs that remove large food groups without reintroduction. | Bloating, gas, and food-trigger patterns, especially when supplements alone do not explain symptoms. |
Safety: Red Flags, Pregnancy, Interactions, and When Supplements Are the Wrong Next Step
IBS is common, but not every bowel symptom is IBS. A clinician should evaluate symptoms such as rectal bleeding, black stool, iron-deficiency anemia, unexplained weight loss, persistent fever, nighttime diarrhea, progressive pain, repeated vomiting, dehydration, new bowel changes after age 50, or a family history of colorectal cancer, inflammatory bowel disease, or celiac disease. These features can point toward conditions that need testing rather than supplement experimentation.[1][9]
Pregnancy and breastfeeding deserve extra caution. Digestive symptoms may change during pregnancy, and supplement safety data are often limited. Peppermint oil, probiotics, PHGG, and psyllium are not the same from a risk standpoint, and product quality varies. People who are pregnant, trying to become pregnant, breastfeeding, immunocompromised, medically complex, taking multiple medications, or caring for a child with IBS-like symptoms should involve a qualified clinician or pharmacist before using supplements.
Medication interactions and timing also matter. Psyllium can affect how some medications are absorbed if taken together. Peppermint oil can worsen reflux and may interact with acid-suppressing strategies or products designed around enteric coating. Probiotics are usually well tolerated by healthy adults but are not risk-free in severely ill or immunocompromised people. A “natural” label does not remove the need for safety checks.[10][11][12]
How to Think About a Supplement Trial Without Overdoing It
IBS supplement decisions are easier to interpret when only one variable changes at a time. Changing peppermint oil, fiber, probiotics, caffeine, dairy, FODMAP intake, stress routines, and medications all at once can make it impossible to know what helped or what caused bloating, constipation, diarrhea, or pain. Clinicians and dietitians often rely on structured symptom tracking because IBS naturally fluctuates.
A useful evidence-based mindset is to define the target symptom before choosing the product. If the main problem is cramping, peppermint oil has a clearer rationale than psyllium. If the main problem is hard stool and incomplete evacuation, soluble fiber is more relevant than a probiotic. If the main problem is bloating after specific foods, a low-FODMAP evaluation or dietitian-guided food assessment may be more useful than adding another microbiome product.[1][2]
There is also a stopping rule: a supplement that clearly worsens symptoms, triggers reflux, increases urgent diarrhea, causes severe bloating, or creates new symptoms should not be kept simply because it is marketed for IBS. Persistent symptoms may require prescription options, dietitian-led therapy, pelvic-floor evaluation, gut-directed psychological therapy, or testing for another condition depending on the pattern.
Bottom Line
For IBS pain and cramping, enteric-coated peppermint oil has the clearest supplement rationale. For IBS-C and mixed stool patterns, psyllium has stronger guideline support than most supplement categories because it is a soluble fiber that can improve stool form. For probiotics, the evidence is more inconsistent: some strains may help some symptoms in some people, but broad “best probiotic for IBS” claims are usually stronger than the data.
PHGG belongs in the conversation as a soluble fiber option, especially when psyllium is poorly tolerated, but it should be presented as an additional fiber choice rather than the main headline comparison. The best approach is subtype-based, symptom-based, and safety-aware: match the supplement to the problem, avoid cure language, watch for red flags, and treat IBS as a gut-brain disorder with multiple possible drivers rather than a condition solved by one product.
FAQ
What is the best supplement for IBS-C?
Among peppermint oil, psyllium, and probiotics, psyllium is usually the most relevant for IBS-C because it is a soluble fiber that can support stool form and regularity. PHGG may be another soluble fiber option for people who do not tolerate psyllium well.[1]
What is the best supplement for IBS-D?
There is no single best supplement for IBS-D. Peppermint oil may be relevant when diarrhea comes with cramping or pain, while psyllium may help stool consistency in some people. Persistent diarrhea or alarm symptoms should be evaluated medically.
Is peppermint oil better than probiotics for IBS?
For short-term abdominal pain and cramping, peppermint oil has a clearer evidence signal than broad probiotic use. Probiotic effects are strain-specific and inconsistent, so one probiotic study cannot be generalized to every product.[5][7]
Can psyllium make IBS bloating worse?
Yes. Psyllium can cause gas, bloating, fullness, or cramping, especially if increased too quickly, taken without enough fluid, or combined with poorly tolerated additives. Tolerance varies from person to person.
Is PHGG the same as psyllium?
No. PHGG is partially hydrolyzed guar gum, while psyllium comes from Plantago ovata husk. Both are soluble fiber options, but they differ in texture, viscosity, fermentation, and available IBS evidence.
Are probiotics safe for IBS?
Many healthy adults tolerate probiotics, but they can cause gas or bloating and are not risk-free for people who are severely ill, immunocompromised, or medically complex. Safety depends on the person and the product.[11]
References
- Lacy, B. E., Pimentel, M., Brenner, D. M., Chey, W. D., Keefer, L. A., Long, M. D., Moshiree, B., & Spiegel, B. M. R. (2021). ACG clinical guideline: Management of irritable bowel syndrome. The American Journal of Gastroenterology, 116(1), 17–44.
- Vasant, D. H., Paine, P. A., Black, C. J., Houghton, L. A., Everitt, H. A., Corsetti, M., Agrawal, A., Aziz, I., Farmer, A. D., Eugenicos, M. P., Moss-Morris, R., Yiannakou, Y., & Ford, A. C. (2021). British Society of Gastroenterology guidelines on the management of irritable bowel syndrome. Gut, 70(7), 1214–1240.
- Drossman, D. A., & Hasler, W. L. (2016). Rome IV—Functional GI disorders: Disorders of gut-brain interaction. Gastroenterology, 150(6), 1257–1261.
- Ford, A. C., Talley, N. J., Spiegel, B. M. R., Foxx-Orenstein, A. E., Schiller, L., Quigley, E. M. M., & Moayyedi, P. (2008). Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: Systematic review and meta-analysis. BMJ, 337, a2313.
- Ingrosso, M. R., Ianiro, G., Nee, J., Lembo, A. J., & Moayyedi, P. (2022). Systematic review and meta-analysis: Efficacy of peppermint oil in irritable bowel syndrome. Alimentary Pharmacology & Therapeutics, 56(6), 932–941.
- Ford, A. C., Harris, L. A., Lacy, B. E., Quigley, E. M. M., & Moayyedi, P. (2018). Systematic review with meta-analysis: The efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Alimentary Pharmacology & Therapeutics, 48(10), 1044–1060.
- Su, G. L., Ko, C. W., Bercik, P., Falck-Ytter, Y., Sultan, S., Weizman, A. V., Morgan, R. L., & the AGA Clinical Guidelines Committee. (2020). AGA clinical practice guidelines on the role of probiotics in the management of gastrointestinal disorders. Gastroenterology, 159(2), 697–705.
- National Institute for Health and Care Excellence. (2017). Irritable bowel syndrome in adults: Diagnosis and management (Clinical guideline CG61).
- National Institute of Diabetes and Digestive and Kidney Diseases. (n.d.). Irritable bowel syndrome. National Institutes of Health.
- National Center for Complementary and Integrative Health. (2025). Peppermint oil. National Institutes of Health.
- National Center for Complementary and Integrative Health. (2025). Probiotics: Usefulness and safety. National Institutes of Health.
- MedlinePlus. (n.d.). Psyllium. U.S. National Library of Medicine.
- Niv, E., Halak, A., Tiommny, E., Yanai, H., Strul, H., Naftali, T., & Vaisman, N. (2006). Role of partially hydrolyzed guar gum in the treatment of irritable bowel syndrome. Nutrition, 22(3), 334–342.